

Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults: An updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care Group
- PMID: 36370077
- PMCID: PMC10107355
- DOI: 10.1111/dme.15005
Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults: An updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care Group
Abstract
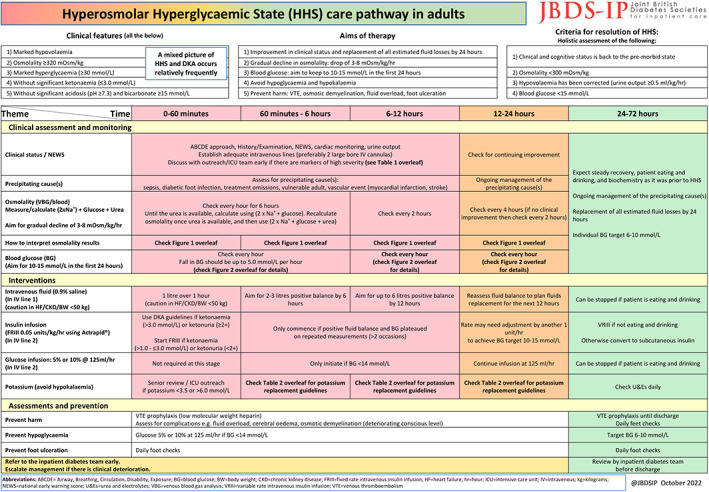
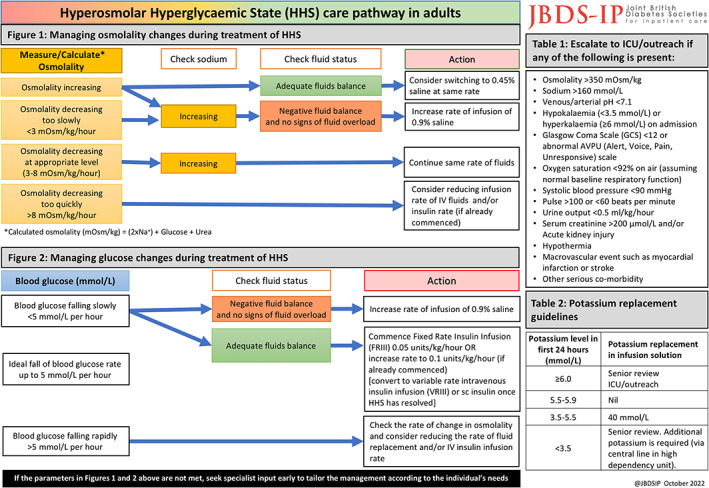
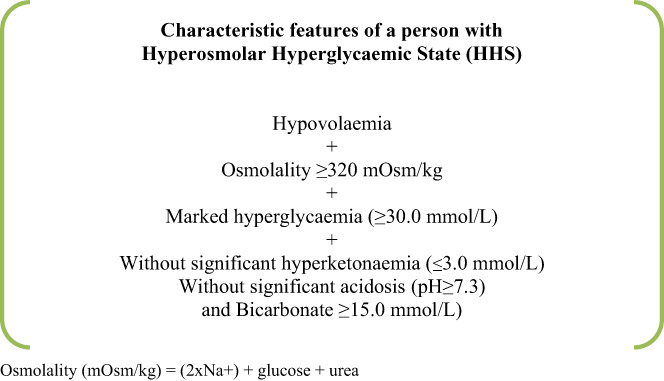
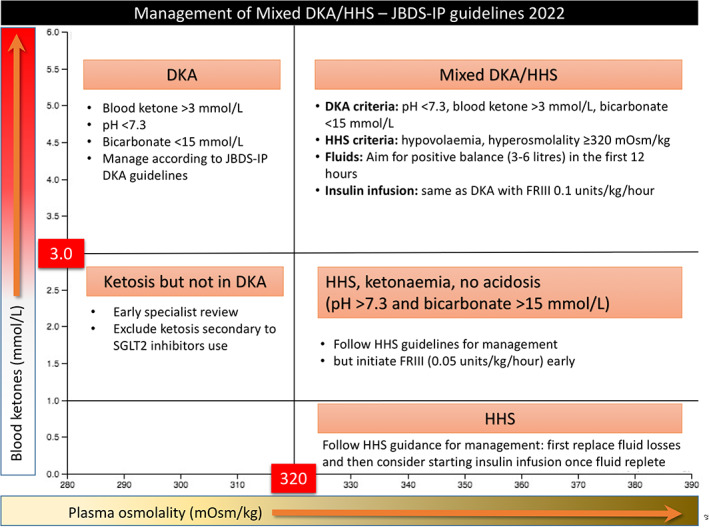
Hyperosmolar Hyperglycaemic State (HHS) is a medical emergency associated with high mortality. It occurs less frequently than diabetic ketoacidosis (DKA), affects those with pre-existing/new type 2 diabetes mellitus and increasingly affecting children/younger adults. Mixed DKA/HHS may occur. The JBDS HHS care pathway consists of 3 themes (clinical assessment and monitoring, interventions, assessments and prevention of harm) and 5 phases of therapy (0-60 min, 1-6, 6-12, 12-24 and 24-72 h). Clinical features of HHS include marked hypovolaemia, osmolality ≥320 mOsm/kg using [(2×Na+ ) + glucose+urea], marked hyperglycaemia ≥30 mmol/L, without significant ketonaemia (≤3.0 mmol/L), without significant acidosis (pH >7.3) and bicarbonate ≥15 mmol/L. Aims of the therapy are to improve clinical status/replace fluid losses by 24 h, gradual decline in osmolality (3.0-8.0 mOsm/kg/h to minimise the risk of neurological complications), blood glucose 10-15 mmol/L in the first 24 h, prevent hypoglycaemia/hypokalaemia and prevent harm (VTE, osmotic demyelination, fluid overload, foot ulceration). Underlying precipitants must be identified and treated. Interventions include: (1) intravenous (IV) 0.9% sodium chloride to restore circulating volume (fluid losses 100-220 ml/kg, caution in elderly), (2) fixed rate intravenous insulin infusion (FRIII) should be commenced once osmolality stops falling with fluid replacement unless there is ketonaemia (FRIII should be commenced at the same time as IV fluids). (3) glucose infusion (5% or 10%) should be started once glucose <14 mmol/L and (4) potassium replacement according to potassium levels. HHS resolution criteria are: osmolality <300 mOsm/kg, hypovolaemia corrected (urine output ≥0.5 ml/kg/h), cognitive status returned to pre-morbid state and blood glucose <15 mmol/L.
Keywords: HHS; emergency; hyperosmolar hyperglycaemic state; inpatient.
© 2022 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK.
Conflict of interest statement
OM has received honoraria, travel and personal fees from Sanofi Diabetes, Eli Lilly, Boehringer Ingelheim and Novo Nordisk. MH has received honoraria, travel and personal fees from Eli Lilly, Astra Zeneca, Novo Nordisk, NAPP, Sanofi and Boehringer Ingelheim. UD has received honoraria and speaker fee from Sanofi Diabetes, Eli Lillly, Astra Zeneca, Boehringer Ingelheim and Novo Nordisk. KD is the chair of the Joint British Diabetes Societies for Inpatient Care and has received honoraria, travel and personal fees from Sanofi Diabetes, Eli Lilly, AstraZeneca, Boehringer Ingelheim and Novo Nordisk.
Figures
Comment in
-
Tonicity or serum osmolality? Comment on management of hyperosmolar hyperglycaemic state in adults: An updated guideline from the Joint British Diabetes Societies for Inpatient Care Group.Diabet Med. 2023 Nov;40(11):e15211. doi: 10.1111/dme.15211. Epub 2023 Sep 3. Diabet Med. 2023. PMID: 37634208 No abstract available.
References
-
- Benoit SR, Hora I, Pasquel FJ, Gregg EW, Albright AL, Imperatore G. Trends in emergency department visits and inpatient admissions for hyperglycemic crises in adults with diabetes in the U.S., 2006–2015. Diabetes Care. 2020;43(5):1057‐1064. http://care.diabetesjournals.org/content/43/5/1057.abstract - PMC - PubMed
-
- Rosenbloom AL. Hyperglycemic hyperosmolar state: an emerging pediatric problem. J Pediatr. 2010;156(2):180‐184. - PubMed
-
- Ekpebegh CO, Longo‐Mbenza B, Akinrinmade A, Blanco‐Blanco E, Bardi M, Levitt NS. Hyperglycaemic crisis in the eastern cape province of South Africa: high mortality and association of hyperosmolar ketoacidosis with a new diagnosis of diabetes. S Afr Med J. 2010;100(12):822‐826. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
