

Nationwide differences in cytology fixation and processing methods and their impact on interlaboratory variation in PD-L1 positivity
- PMID: 36370167
- PMCID: PMC10067664
- DOI: 10.1007/s00428-022-03446-w
Nationwide differences in cytology fixation and processing methods and their impact on interlaboratory variation in PD-L1 positivity
Abstract
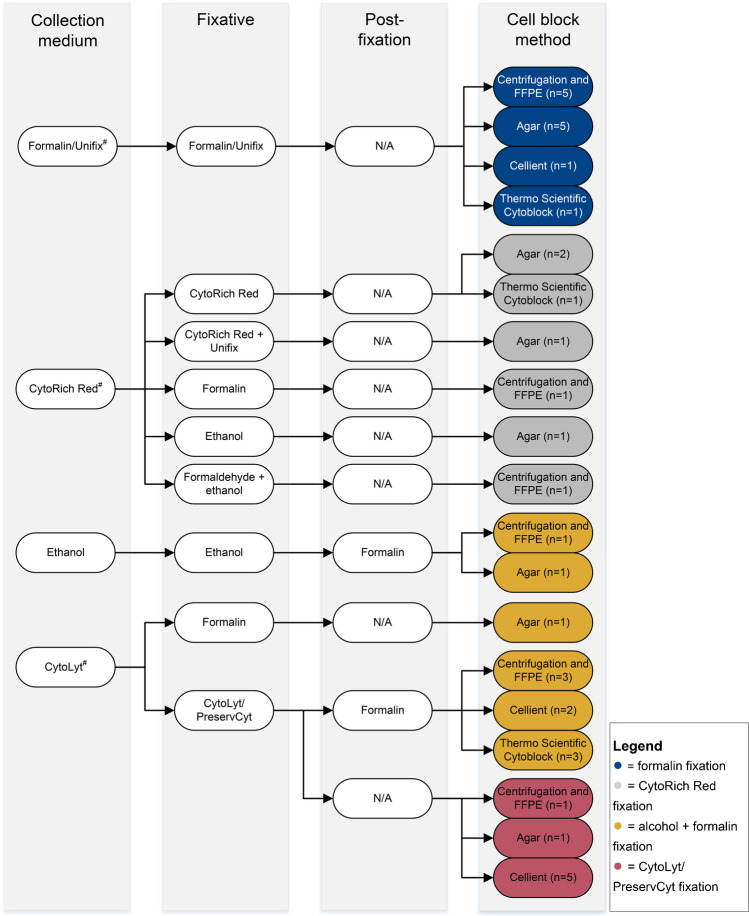
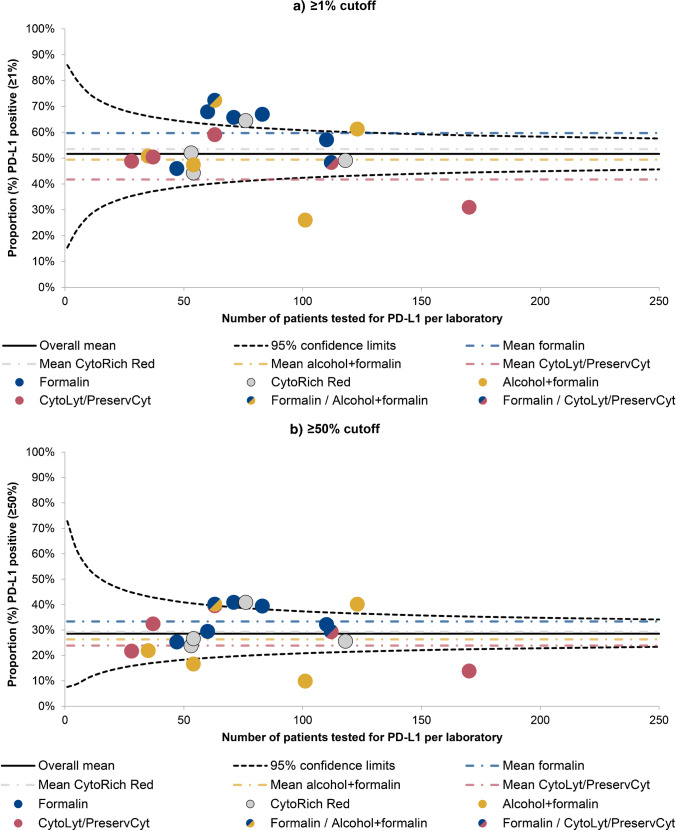
Programmed death ligand-1 (PD-L1) immunostaining, which aids clinicians in decision-making on immunotherapy for non-small cell lung cancer (NSCLC) patients, is sometimes performed on cytological specimens. In this study, differences in cytology fixation and cell block (CB) processing between pathology laboratories were assessed, and the influence of these differences on interlaboratory variation in PD-L1 positivity was investigated. Questionnaires on cytology processing were sent to all Dutch laboratories. Information gathered from the responses was added to data on all Dutch NSCLC patients with a mention of PD-L1 testing in their cytopathology report from July 2017 to December 2018, retrieved from PALGA (the nationwide network and registry of histo- and cytopathology in the Netherlands). Case mix-adjusted PD-L1 positivity rates were determined for laboratories with known fixation and CB method. The influence of differences in cytology processing on interlaboratory variation in PD-L1 positivity was assessed by comparing positivity rates adjusted for differences in the variables fixative and CB method with positivity rates not adjusted for differences in these variables. Twenty-eight laboratories responded to the survey and reported 19 different combinations of fixation and CB method. Interlaboratory variation in PD-L1 positivity was assessed in 19 laboratories. Correcting for differences in the fixative and CB method resulted in a reduction (from eight (42.1%) to five (26.3%)) in the number of laboratories that differed significantly from the mean in PD-L1 positivity. Substantial variation in cytology fixation and CB processing methods was observed between Dutch pathology laboratories, which partially explains the existing considerable interlaboratory variation in PD-L1 positivity.
Keywords: Cytological techniques; Fixatives; Immunocytochemistry; Interlaboratory variation; Non-small cell lung cancer; Programmed death ligand-1.
© 2022. The Author(s).
Conflict of interest statement
This work was funded with research grants from AstraZeneca, MSD, and Roche (grant numbers not applicable), received by BM Koomen and SM Willems, and paid to the institution. None of the grant suppliers was involved in the study design, collection, analysis and interpretation of data, writing of the manuscript, or the decision to submit the manuscript for publication. SM Willems also received research grants from Amgen, AstraZeneca, Bayer, MSD, Novartis, Pfizer, and Roche, all outside the submitted work and paid to the institution. The other authors declare no conflict of interest.
Figures


Comment in
-
Comments to: Nationwide differences in cytology fixation and processing methods and their impact on interlaboratory variation in PD-L1 positivity.Virchows Arch. 2023 Apr;482(4):797-798. doi: 10.1007/s00428-023-03503-y. Epub 2023 Feb 2. Virchows Arch. 2023. PMID: 36729182 No abstract available.
References
-
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391(10125):1023–1075. doi: 10.1016/S0140-6736(17)33326-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
