

Comparative accuracy of biomarkers for the prediction of hospital-acquired acute kidney injury: a systematic review and meta-analysis
- PMID: 36371256
- PMCID: PMC9652605
- DOI: 10.1186/s13054-022-04223-6
Comparative accuracy of biomarkers for the prediction of hospital-acquired acute kidney injury: a systematic review and meta-analysis
Abstract
Background: Several biomarkers have been proposed to predict the occurrence of acute kidney injury (AKI); however, their efficacy varies between different trials. The aim of this study was to compare the predictive performance of different candidate biomarkers for AKI.
Methods: In this systematic review, we searched PubMed, Medline, Embase, and the Cochrane Library for papers published up to August 15, 2022. We selected all studies of adults (> 18 years) that reported the predictive performance of damage biomarkers (neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), liver-type fatty acid-binding protein (L-FABP)), inflammatory biomarker (interleukin-18 (IL-18)), and stress biomarker (tissue inhibitor of metalloproteinases-2 × insulin-like growth factor-binding protein-7 (TIMP-2 × IGFBP-7)) for the occurrence of AKI. We performed pairwise meta-analyses to calculate odds ratios (ORs) and 95% confidence intervals (CIs) individually. Hierarchical summary receiver operating characteristic curves (HSROCs) were used to summarize the pooled test performance, and the Grading of Recommendations, Assessment, Development and Evaluations criteria were used to appraise the quality of evidence.
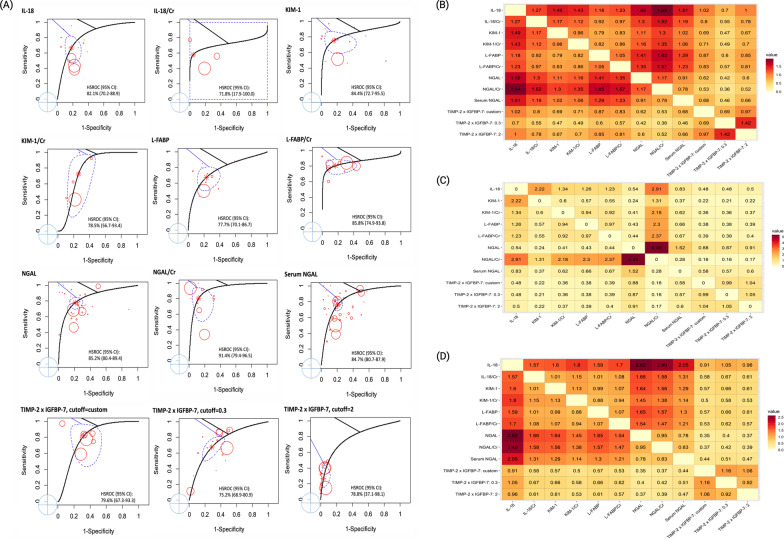
Results: We identified 242 published relevant studies from 1,803 screened abstracts, of which 110 studies with 38,725 patients were included in this meta-analysis. Urinary NGAL/creatinine (diagnostic odds ratio [DOR] 16.2, 95% CI 10.1-25.9), urinary NGAL (DOR 13.8, 95% CI 10.2-18.8), and serum NGAL (DOR 12.6, 95% CI 9.3-17.3) had the best diagnostic accuracy for the risk of AKI. In subgroup analyses, urinary NGAL, urinary NGAL/creatinine, and serum NGAL had better diagnostic accuracy for AKI than urinary IL-18 in non-critically ill patients. However, all of the biomarkers had similar diagnostic accuracy in critically ill patients. In the setting of medical and non-sepsis patients, urinary NGAL had better predictive performance than urinary IL-18, urinary L-FABP, and urinary TIMP-2 × IGFBP-7: 0.3. In the surgical patients, urinary NGAL/creatinine and urinary KIM-1 had the best diagnostic accuracy. The HSROC values of urinary NGAL/creatinine, urinary NGAL, and serum NGAL were 91.4%, 85.2%, and 84.7%, respectively.
Conclusions: Biomarkers containing NGAL had the best predictive accuracy for the occurrence of AKI, regardless of whether or not the values were adjusted by urinary creatinine, and especially in medically treated patients. However, the predictive performance of urinary NGAL was limited in surgical patients, and urinary NGAL/creatinine seemed to be the most accurate biomarkers in these patients. All of the biomarkers had similar predictive performance in critically ill patients. Trial registration CRD42020207883 , October 06, 2020.
Keywords: Acute kidney injury; Biomarker; Critically ill patient; Neutrophil gelatinase-associated lipocalin.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- MOST 108-2321-B-182-003/Ministry of Science and Technology (MOST) of the Republic of China (Taiwan)
- MOST 109-2321-B-182-001/Ministry of Science and Technology (MOST) of the Republic of China (Taiwan)
- MOST 106-2321-B-182-002/Ministry of Science and Technology (MOST) of the Republic of China (Taiwan)
- MOST 107-2321-B-182-004/Ministry of Science and Technology (MOST) of the Republic of China (Taiwan)
- 104-2314-B-002-125-MY3/National Science Council
- 106-2314-B-002 -166 -MY3/National Science Council
- 107-2314-B-002-026-MY3/National Science Council
- PH-102-SP-09/National Health Research Institutes
- 106-FTN20/National Taiwan University Hospital
- 106-P02/National Taiwan University Hospital
- UN106-014/National Taiwan University Hospital
- 106-S3582/National Taiwan University Hospital
- 107-S3809/National Taiwan University Hospital
- 107-T02/National Taiwan University Hospital
- PC1246/National Taiwan University Hospital
- VN109-09/National Taiwan University Hospital
- 109-S4634/National Taiwan University Hospital
- UN109-041/National Taiwan University Hospital
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
