

Comprehensive genetic and functional analyses of Fc gamma receptors influence on response to rituximab therapy for autoimmunity
- PMID: 36371989
- PMCID: PMC9663864
- DOI: 10.1016/j.ebiom.2022.104343
Comprehensive genetic and functional analyses of Fc gamma receptors influence on response to rituximab therapy for autoimmunity
Abstract
Background: Rituximab is widely used to treat autoimmunity but clinical response varies. Efficacy is determined by the efficiency of B-cell depletion, which may depend on various Fc gamma receptor (FcγR)-dependent mechanisms. Study of FcγR is challenging due to the complexity of the FCGR genetic locus. We sought to assess the effect of FCGR variants on clinical response, B-cell depletion and NK-cell-mediated killing in rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).
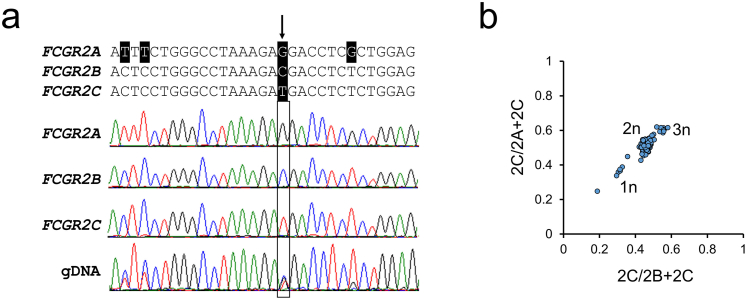
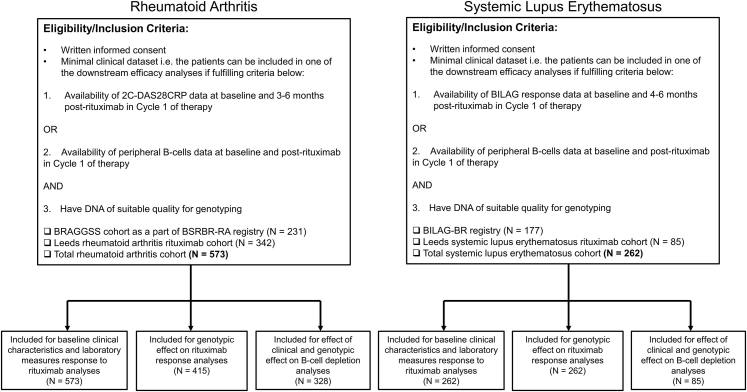
Methods: A longitudinal cohort study was conducted in 835 patients [RA = 573; SLE = 262]. Clinical outcome measures were two-component disease activity score in 28-joints (2C-DAS28CRP) for RA and British Isles Lupus Assessment Group (BILAG)-2004 major clinical response (MCR) for SLE at 6 months. B-cells were evaluated by highly-sensitive flow cytometry. Single nucleotide polymorphism and copy number variation for genes encoding five FcγRs were measured using multiplex ligation-dependent probe amplification. Ex vivo studies assessed NK-cell antibody-dependent cellular cytotoxicity (ADCC) and FcγR expression.
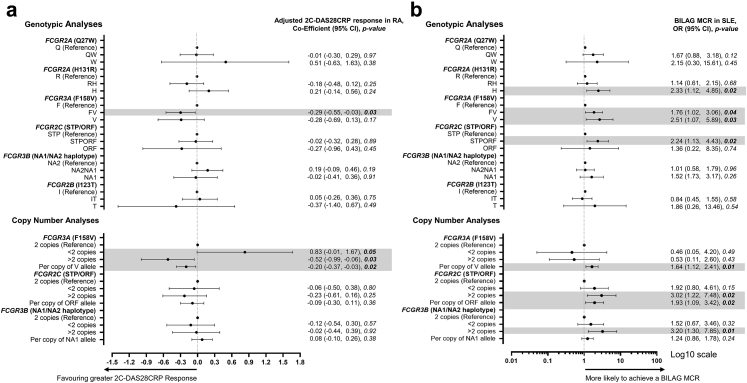
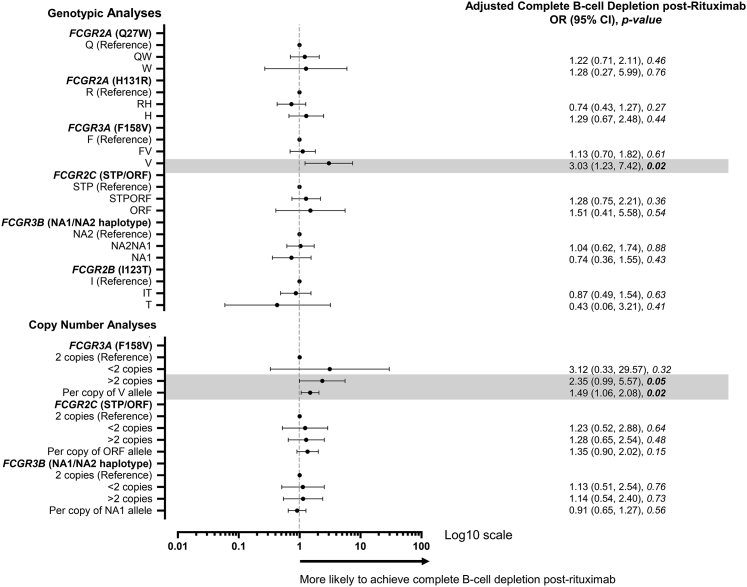
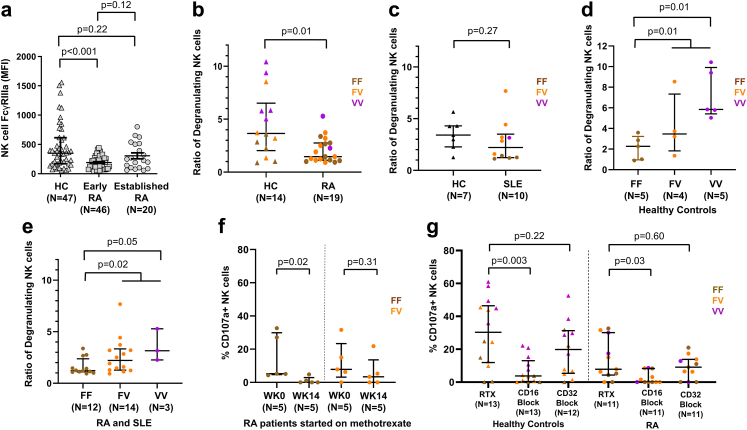
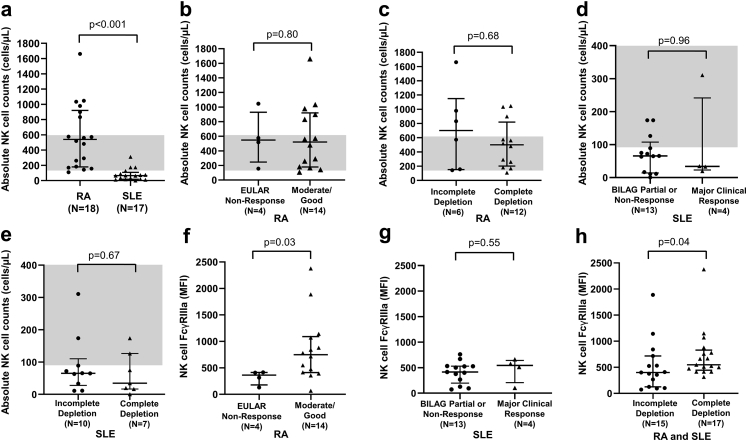
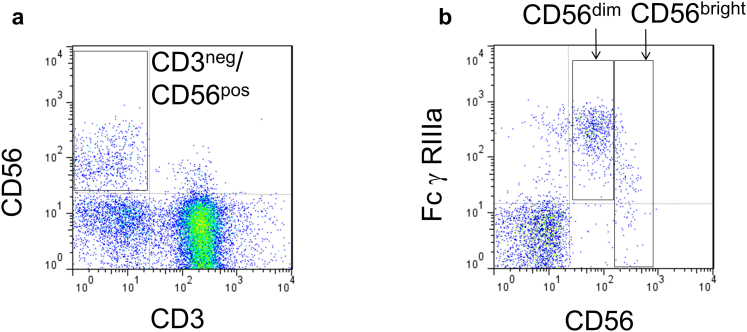
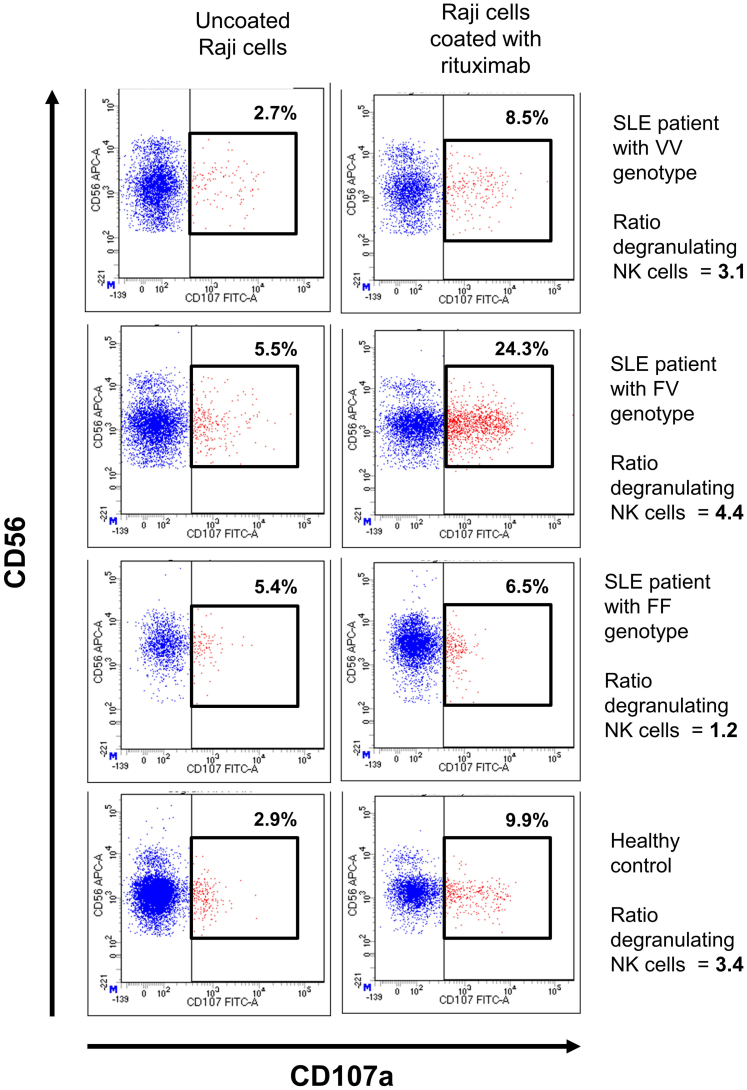
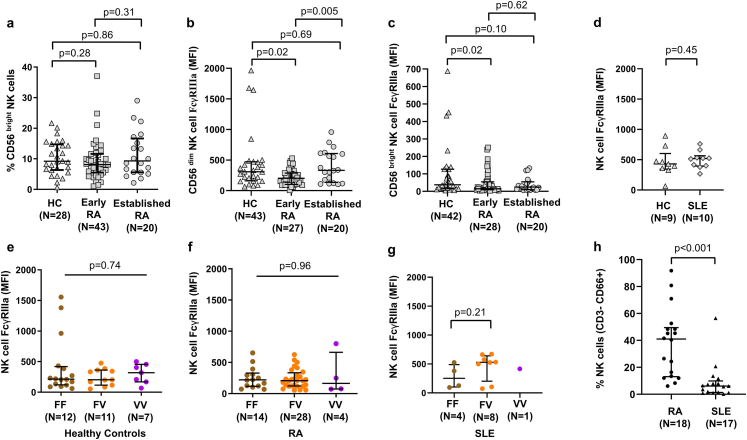
Findings: In RA, carriage of FCGR3A-158V and increased FCGR3A-158V copies were associated with greater 2C-DAS28CRP response (adjusted for baseline 2C-DAS28CRP). In SLE, MCR was associated with increased FCGR3A-158V, OR 1.64 (95% CI 1.12-2.41) and FCGR2C-ORF OR 1.93 (95% CI 1.09-3.40) copies. 236/413 (57%) patients with B-cell data achieved complete depletion. Homozygosity for FCGR3A-158V and increased FCGR3A-158V copies were associated with complete depletion in combined analyses. FCGR3A genotype was associated with rituximab-induced ADCC, and increased NK-cell FcγRIIIa expression was associated with improved clinical response and depletion in vivo. Furthermore, disease status and concomitant therapies impacted both NK-cell FcγRIIIa expression and ADCC.
Interpretation: FcγRIIIa is the major low affinity FcγR associated with rituximab response. Increased copies of the FCGR3A-158V allele (higher affinity for IgG1), influences clinical and biological responses to rituximab in autoimmunity. Enhancing FcγR-effector functions could improve the next generation of CD20-depleting therapies and genotyping may stratify patients for optimal treatment protocols.
Funding: Medical Research Council, National Institute for Health and Care Research, Versus Arthritis.
Keywords: Autoimmune diseases; B-lymphocytes; Genetics; Rheumatoid arthritis; Rituximab; Systemic lupus erythematosus.
Copyright © 2022 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests Prof Bruce has received research grants from GSK, consulting fees from GSK, UCB, Eli Lilly & Co, BMS, Aurinia, IL-TOO and AstraZeneca and speaker fees from AstraZeneca, GSK and UCB within the last 3 years. Dr Vital has received honoraria and consulting fees from Roche within the last 3 years. All other authors declare no competing interest related to the work described in this manuscript.
Figures
References
-
- Garcia-Montoya L., Villota-Eraso C., Yusof M.Y.M., Vital E.M., Emery P. Lessons for rituximab therapy in patients with rheumatoid arthritis. Lancet Rheumatol. 2020;2(8):e497–e509. - PubMed
-
- Fanouriakis A., Kostopoulou M., Alunno A., et al. 2019 Update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736–745. - PubMed
-
- Ramos-Casals M., Soto M.J., Cuadrado M.J., Khamashta M.A. Rituximab in systemic lupus erythematosus: a systematic review of off-label use in 188 cases. Lupus. 2009;18(9):767–776. - PubMed
-
- Dass S., Rawstron A.C., Vital E.M., Henshaw K., McGonagle D., Emery P. Highly sensitive B cell analysis predicts response to rituximab therapy in rheumatoid arthritis. Arthritis Rheum. 2008;58(10):2993–2999. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
