

Serum GFAP and NfL Levels Differentiate Subsequent Progression and Disease Activity in Patients With Progressive Multiple Sclerosis
- PMID: 36376097
- PMCID: PMC9749933
- DOI: 10.1212/NXI.0000000000200052
Serum GFAP and NfL Levels Differentiate Subsequent Progression and Disease Activity in Patients With Progressive Multiple Sclerosis
Abstract
Background and objectives: Neurodegeneration and astrocytic activation are pathologic hallmarks of progressive multiple sclerosis (MS) and can be quantified by serum neurofilament light chain (sNfL) and glial fibrillary acidic protein (sGFAP). We investigated sNfL and sGFAP as tools for stratifying patients with progressive MS based on progression and disease activity status.
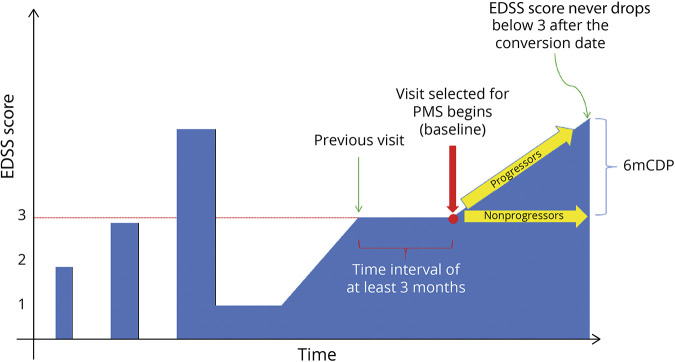
Methods: We leveraged our Comprehensive Longitudinal Investigation of MS at the Brigham and Women's Hospital (CLIMB) natural history study, which includes clinical, MRI data and serum samples collected over more than 20 years. We included patients with MS with a confirmed Expanded Disability Status Scale (EDSS) score ≥3 that corresponds with our classifier for patients at high risk of underlying progressive pathology. We analyzed sNfL and sGFAP within 6 months from the confirmed EDSS score ≥3 corresponding with our baseline visit. Patients who further developed 6-month confirmed disability progression (6mCDP) were classified as progressors. We further stratified our patients into active/nonactive based on new brain/spinal cord lesions or relapses in the 2 years before baseline or during follow-up. Statistical analysis on log-transformed sGFAP/sNfL assessed the baseline association with demographic, clinical, and MRI features and associations with future disability.
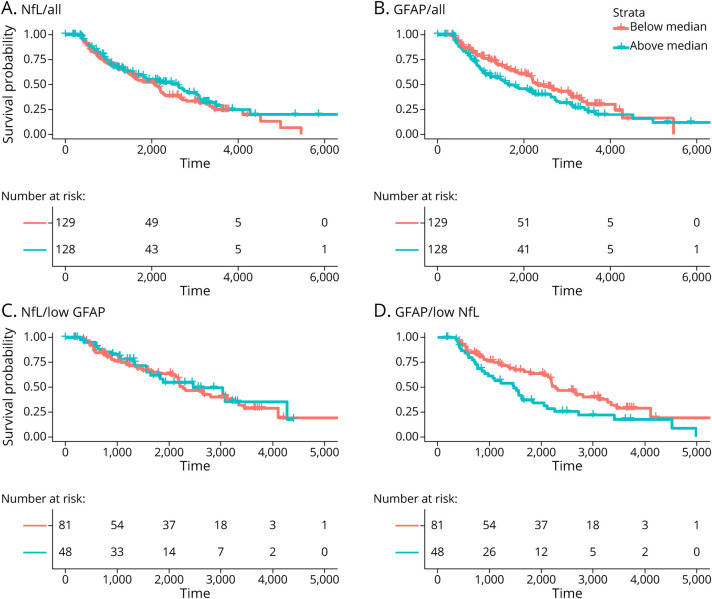
Results: We included 257 patients with MS who had an average EDSS score of 4.0 and a median follow-up after baseline of 7.6 years. sNfL was higher in patients with disease activity in the 2 years before baseline (adjusted β = 1.21; 95% CI 1.04-1.42; p = 0.016), during the first 2 years of follow-up (adjusted β = 1.17; 95% CI = 1.01-1.36; p = 0.042). sGFAP was not increased in the presence of disease activity. Higher sGFAP levels, but not sNfL levels, were associated with higher risk of 6mCDP (adjusted hazard ratio [HR] = 1.71; 95% CI = 1.19-2.45; p = 0.004). The association was stronger in patients with low sNfL (adjusted HR = 2.44; 95% CI 1.32-4.52; p = 0.005) and patients who were nonactive in the 2 years prior or after the sample.
Discussion: Higher levels of sGFAP correlated with subsequent progression, particularly in nonactive patients, whereas sNfL reflected acute disease activity in patients with MS at high risk of underlying progressive pathology. Thus, sGFAP and sNfL levels may be used to stratify patients with progressive MS for clinical research studies and clinical trials and may inform clinical care.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous