

Racial disparities and prevalence of cardiovascular disease risk factors, cardiometabolic risk factors, and cardiovascular health metrics among US adults: NHANES 2011-2018
- PMID: 36376533
- PMCID: PMC9663590
- DOI: 10.1038/s41598-022-21878-x
Racial disparities and prevalence of cardiovascular disease risk factors, cardiometabolic risk factors, and cardiovascular health metrics among US adults: NHANES 2011-2018
Abstract
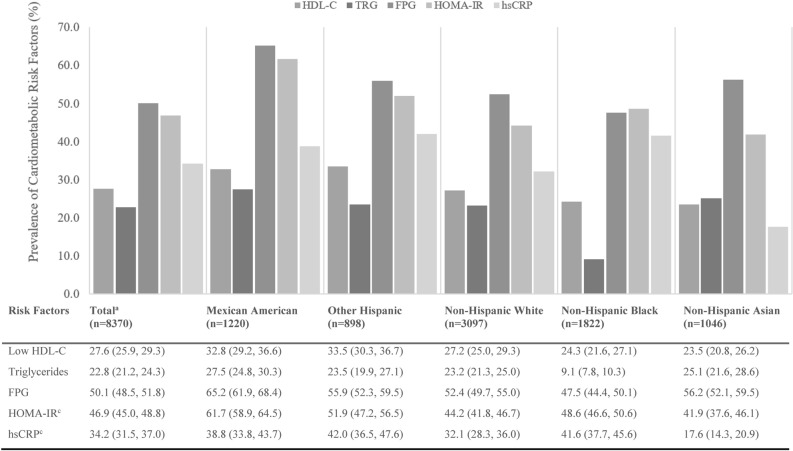
This study estimated the prevalence of cardiovascular disease (CVD) risk factors, cardiometabolic (CM) risk factors, and cardiovascular health metrics (CVHMs) among US adults and across race/ethnicity groups. The study comprised 8370 US adults aged ≥ 20 years from the National Health and Nutrition Examination Survey (NHANES) 2011-2018, free of coronary heart disease/heart failure, angina/angina pectoris, heart attack, and stroke, who provided complete data for the outcome variables of interest. Age-adjusted prevalence of CVD and CM risk factors, and CVHMs were computed for all adults and across race/ethnicity groups. All analyses accounted for the complex, multi-stage survey sampling design of the NHANES. Hypertension (45.0%), obesity (40.0%), fasting plasma glucose ≥ 100 mg/dL or hypoglycemic medication (51.0%), ideal physical activity (59.2%) and ideal smoking status (56.9%) were most prevalent for the whole sample. Mexican Americans and non-Hispanic Blacks had elevated risk for some, but not all, CVD and CM risk factors compared to non-Hispanic Whites and non-Hispanic Asians. Reducing further health disparities and persisting differences among racial and ethnic groups is vital to achieving the American Heart Association vision of all people having ideal cardiovascular health, living healthier and longer.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
