

Practice of oxygen use in anesthesiology - a survey of the European Society of Anaesthesiology and Intensive Care
- PMID: 36376798
- PMCID: PMC9660141
- DOI: 10.1186/s12871-022-01884-2
Practice of oxygen use in anesthesiology - a survey of the European Society of Anaesthesiology and Intensive Care
Abstract
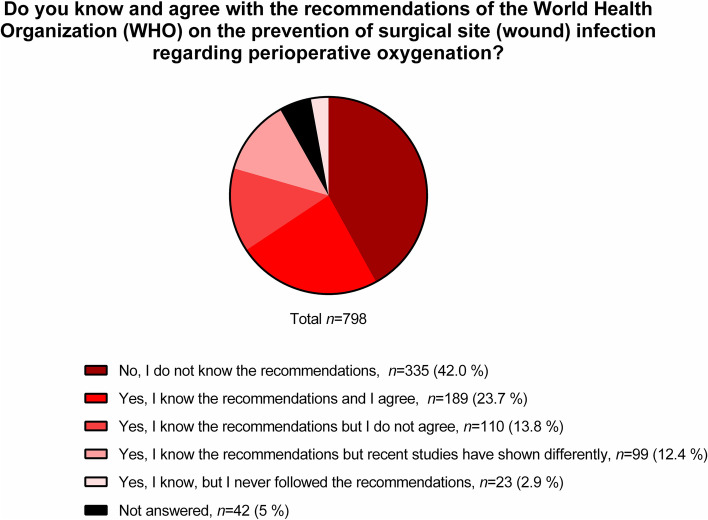
Background: Oxygen is one of the most commonly used drugs by anesthesiologists. The World Health Organization (WHO) gave recommendations regarding perioperative oxygen administration, but the practice of oxygen use in anesthesia, critical emergency, and intensive care medicine remains unclear.
Methods: We conducted an online survey among members of the European Society of Anaesthesiology and Intensive Care (ESAIC). The questionnaire consisted of 46 queries appraising the perioperative period, emergency medicine and in the intensive care, knowledge about current recommendations by the WHO, oxygen toxicity, and devices for supplemental oxygen therapy.
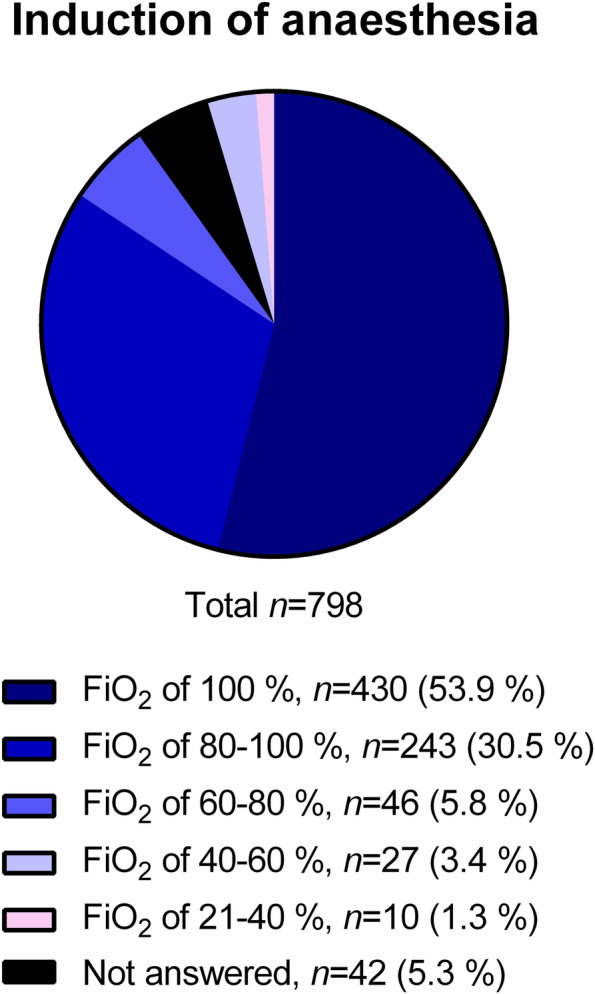
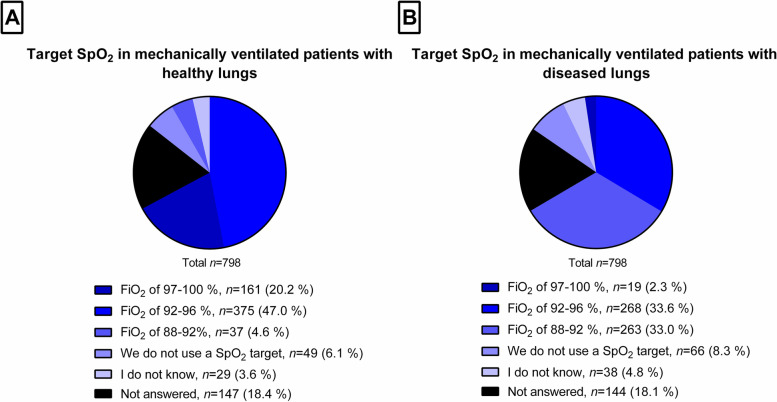
Results: Seven hundred ninety-eight ESAIC members (2.1% of all ESAIC members) completed the survey. Most respondents were board-certified and worked in hospitals with > 500 beds. The majority affirmed that they do not use specific protocols for oxygen administration. WHO recommendations are unknown to 42% of respondents, known but not followed by 14%, and known and followed by 24% of them. Respondents prefer inspiratory oxygen fraction (FiO2) ≥80% during induction and emergence from anesthesia, but intraoperatively < 60% for maintenance, and higher FiO2 in patients with diseased than non-diseased lungs. Postoperative oxygen therapy is prescribed more commonly according to peripheral oxygen saturation (SpO2), but shortage of devices still limits monitoring. When monitoring is used, SpO2 ≤ 95% is often targeted. In critical emergency medicine, oxygen is used frequently in patients aged ≥80 years, or presenting with respiratory distress, chronic obstructive pulmonary disease, myocardial infarction, and stroke. In the intensive care unit, oxygen is mostly targeted at 96%, especially in patients with pulmonary diseases.
Conclusions: The current practice of perioperative oxygen therapy among respondents does not follow WHO recommendations or current evidence, and access to postoperative monitoring devices impairs the individualization of oxygen therapy. Further research and additional teaching about use of oxygen are necessary.
Keywords: Critical emergency medicine; Inspiratory fraction of oxygen; Intensive care medicine; Oxygen therapy; Oxygen toxicity; Patient safety; Perioperative care; Supplemental oxygen; WHO guidelines on surgical site infection prevention.
© 2022. The Author(s).
Conflict of interest statement
Dr. M. Gama de Abreu received consultation fees from Ambu, GE Healthcare, ZOLL and Dräger Medical AG. Dr. K. Krenn reports travel grants from Biotest and a grant from Apeptico GmbH. All other authors (MS, TW, JW, MF, PB, SDH, JFAH, and DI) declared no competing interests.
Figures
References
-
- Hafner C, Wu J, Soto-Gonzalez L, Kaun C, Stojkovic S, Wojta J, et al. Moderate hyperoxia induces inflammation, apoptosis and necrosis in human umbilical vein endothelial cells: an in-vitro study. Eur J Anaesthesiol. 2017;34(3):141–149. - PubMed
-
- Hafner C, Wu J, Tiboldi A, Hess M, Mitulovic G, Kaun C, et al. Hyperoxia induces inflammation and cytotoxicity in human adult cardiac myocytes. Shock Augusta Ga. 2017;47(4):436–444. - PubMed
-
- Barazzone C, Horowitz S, Donati YR, Rodriguez I, Piguet PF. Oxygen toxicity in mouse lung: pathways to cell death. Am J Respir Cell Mol Biol. 1998;19(4):573–581. - PubMed
-
- Hedenstierna G, Rothen HU. Respiratory function during anesthesia: effects on gas exchange. Compr Physiol. 2012;2(1):69–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
