

Bipolar I and bipolar II subtypes in older age: Results from the Global Aging and Geriatric Experiments in Bipolar Disorder (GAGE-BD) project
- PMID: 36377516
- PMCID: PMC10265276
- DOI: 10.1111/bdi.13271
Bipolar I and bipolar II subtypes in older age: Results from the Global Aging and Geriatric Experiments in Bipolar Disorder (GAGE-BD) project
Abstract
Objectives: The distinction between bipolar I disorder (BD-I) and bipolar II disorder (BD-II) has been a topic of long-lasting debate. This study examined differences between BD-I and BD-II in a large, global sample of OABD, focusing on general functioning, cognition and somatic burden as these domains are often affected in OABD.
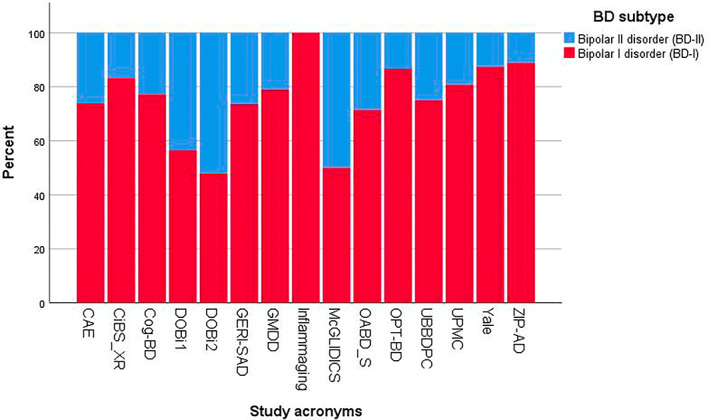
Methods: Cross-sectional analyses were conducted with data from the Global Aging and Geriatric Experiments in Bipolar Disorder (GAGE-BD) database. The sample included 963 participants aged ≥50 years (714 BD-I, 249 BD-II). Sociodemographic and clinical factors were compared between BD subtypes including adjustment for study cohort. Multivariable analyses were conducted with generalized linear mixed models (GLMMs) and estimated associations between BD subtype and (1) general functioning (GAF), (2) cognitive performance (g-score) and (3) somatic burden, with study cohort as random intercept.
Results: After adjustment for study cohort, BD-II patients more often had a late onset ≥50 years (p = 0.008) and more current severe depression (p = 0.041). BD-I patients were more likely to have a history of psychiatric hospitalization (p < 0.001) and current use of anti-psychotics (p = 0.003). Multivariable analyses showed that BD subtype was not related to GAF, cognitive g-score or somatic burden.
Conclusion: BD-I and BD-II patients did not differ in terms of general functioning, cognitive impairment or somatic burden. Some clinical differences were observed between the groups, which could be the consequence of diagnostic definitions. The distinction between BD-I and BD-II is not the best way to subtype OABD patients. Future research should investigate other disease specifiers in this population.
Keywords: bipolar disorder; cognition; comorbidities; diagnostic subtypes; elderly; functioning; geriatrics; impairment; older-age bipolar disorder (OABD); psychiatry.
© 2022 The Authors. Bipolar Disorders published by John Wiley & Sons Ltd.
Conflict of interest statement
Alexandra Beunders, Almar Kok, Sigfried Schouws, Ralph Kupka, Farren Briggs, Lisa Eyler, Orestes Forlenza, Ariel Gildengers, Kaylee Sarna, Ashley Sutherland, Joy Yala, Luca Villa, Nicole Korten and Annemiek Dols have no conflicts to report. Federica Klaus has no conflict of interest to report, but receives an Early. Postdoc Mobility Fellowship of the Swiss National Science Foundation (SNSF) (grant number P2ZHP3_181506) and Novartis Foundation for Medical‐Biological Research Fellowship. Hilary Blumberg received an honorarium from Aetna for a presentation. Brent Forester has received research grants from Biogen, Eisai, The Rogers Family Foundation, The Spier Family Foundation and the National Institutes of Health. He has previously served as a consultant for Acadia Pharmaceuticals and Biogen. He currently serves on the Advisory Board for Patina Health and the Pharmacy and Therapeutics Committee for CVS Health. Esther Jiménez declares no conflict of interest but has a research grant from the Instituto de Salud Carlos III (ISCIII) and the Spanish Ministry of Science and Innovation (PI20/00060)). Benoit Mulsant receives compensation from the Department of Psychiatry, University of Toronto, Toronto, Ontario; the Centre for Addiction and Mental Health (CAMH), Toronto, Ontario; and the University of Pittsburgh, Pennsylvania. Dr Mulsant is a member of the Board of Trustees, Centre for Addiction and Mental Health, Toronto, Ontario. Dr Mulsant currently receives research support from Brain Canada, the Canadian Institutes of Health Research, the CAMH Foundation, the Patient‐Centered Outcomes Research Institute (PCORI), the US National Institute of Health (NIH), Eli Lilly, Pfizer, Capital Solution Design LLC, and HAPPYneuron. He has also received research support from Bristol‐Myers Squibb, Eli Lilly and Pfizer. He directly owns stocks of General Electric. Regan Patrick receives partial salary support from Rogers Family Foundation, Biogen and NIH/NIA. Soham Rej receives salary support from a clinician‐investigator award from the Fonds de Recherche Québec Santé (FRQS) and owns shares in Aifred Health. Martha Sajatovic has received the following research grants within the past 3 years: Nuromate, Otsuka, International Society for Bipolar Disorders (ISBD), National Institutes of Health (NIH), Centers for Disease Control and Prevention (CDC), and Patient‐Centered Outcomes Research Institute (PCORI). In the past year, she has been a consultant for Alkermes, Otsuka, Sunovion, Janssen, Lundbeck, Teva, Clinical Education Alliance, and Health Analytics. In the past year, she received royalties from Springer Press, Johns Hopkins University Press, Oxford Press, and UpToDate. She received compensation for preparation of/participation in CME activities in the past year from the American Physician's Institute (CMEtoGo, Psychopharmacology Institute, Novus, American Epilepsy Society, American Society of Clinical Psychopharmacology, and American Academy of Child and Adolescent Psychiatry. Eduard Vieta has received grants and served as consultant, advisor or CME speaker for the following entities: AB‐Biotics, Abbott, Allergan, Angelini, AstraZeneca, Biogen, Bristol‐Myers Squibb, Celon, Dainippon Sumitomo Pharma, Farmindustria, Ferrer, Forest Research Institute, Gedeon Richter, GH Research, Glaxo‐Smith‐Kline, Janssen, Lundbeck, Otsuka, Pfizer, Roche, Sage, Sanofi‐Aventis, Servier, Shire, Sunovion, Takeda, the Brain and Behaviour Foundation, the Generalitat de Catalunya (PERIS), the Spanish Ministry of Science and Innovation (CIBERSAM), EU Horizon 2020 and the Stanley Medical Research Institute.
Figures
References
-
- American Psychiatric Publishing , ed. Diagnostic and Statistical Manual of Mental Disorders (5th Ed.). American Psychiatric Association; 2013.
