

Clinical and Socioeconomic Determinants of Angiotensin Receptor-Neprilysin Inhibitor Prescription at Hospital Discharge in Patients With Heart Failure With Reduced Ejection Fraction
- PMID: 36378759
- PMCID: PMC9673159
- DOI: 10.1161/CIRCHEARTFAILURE.121.009395
Clinical and Socioeconomic Determinants of Angiotensin Receptor-Neprilysin Inhibitor Prescription at Hospital Discharge in Patients With Heart Failure With Reduced Ejection Fraction
Abstract
Background: Angiotensin receptor-neprilysin inhibitor (ARNI) prescription in the United States remains suboptimal despite strong evidence for efficacy and value in heart failure with reduced ejection fraction. Factors responsible for under prescription are not completely understood. Economic limitations may play a disproportionate role in reduced access for some patients.
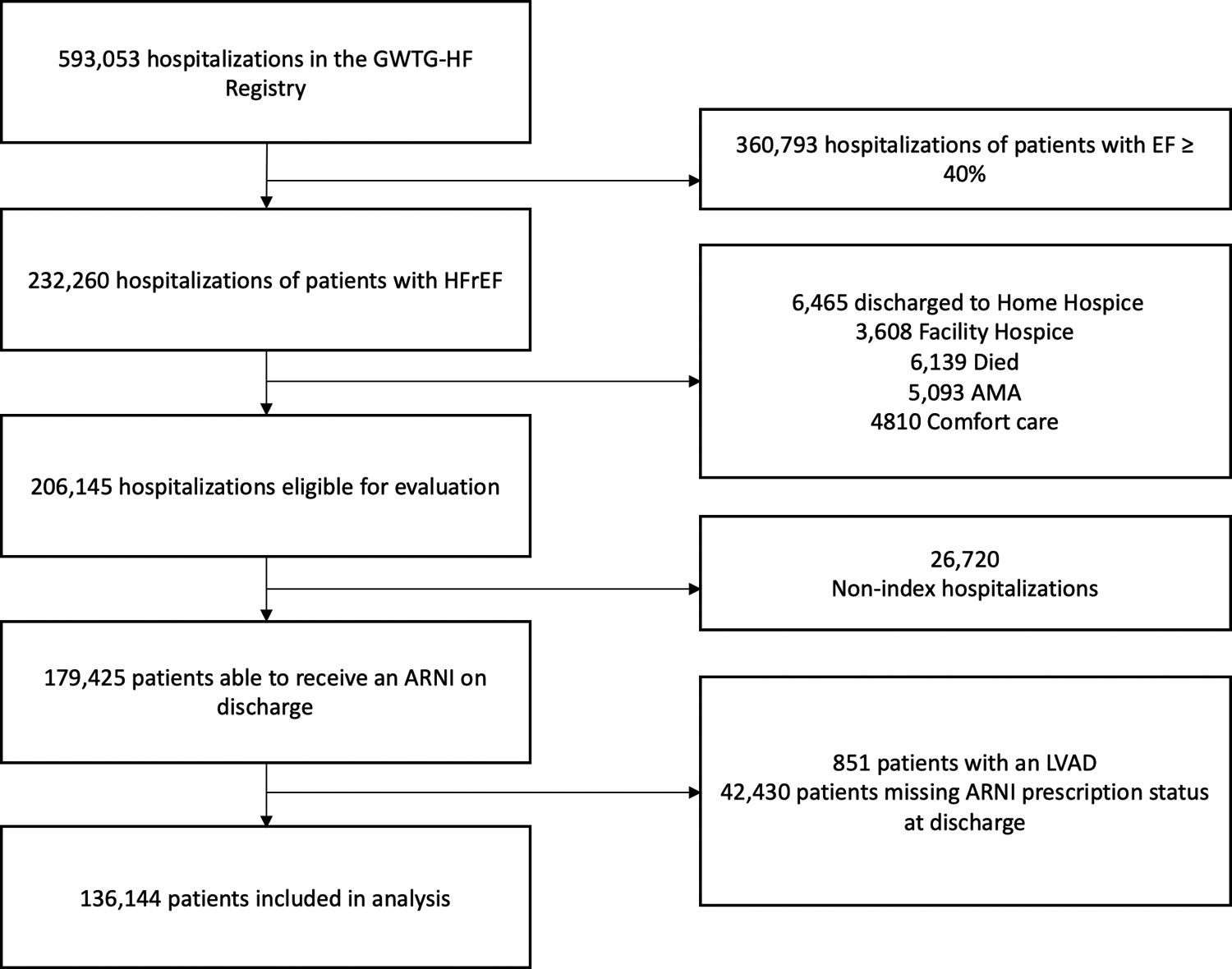
Methods: This is an analysis of the Get With The Guidelines-Heart Failure registry, supplemented with data from the Distressed Community Index. Data were fit to a mixed-effects regression model to investigate clinical and socioeconomic factors associated with ARNI prescription at hospital discharge. Missing data were handled by multilevel multiple imputation.
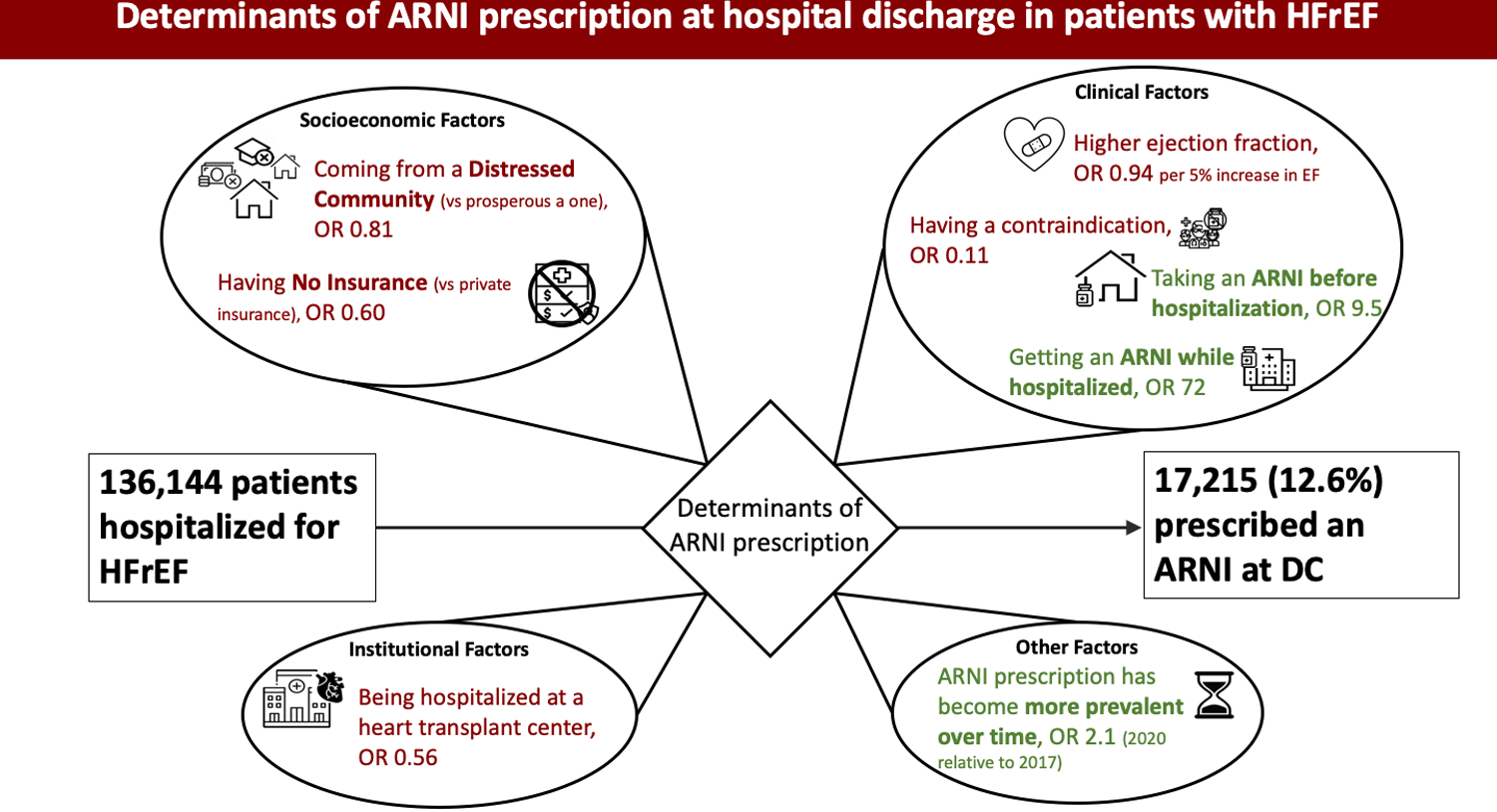
Results: Of the 136 144 patients included in analysis, 12.6% were prescribed an ARNI at discharge. The dominant determinants of ARNI prescription were ARNI use while inpatient (odds ratio [OR], 72 [95% CI, 58-89]; P<0.001) and taking an ARNI before hospitalization (OR 9 [95% CI, 7-13]; P<0.001). Having an ACE (angiotensin-converting enzyme) inhibitor/angiotensin receptor blocker (ARB)/ARNI contraindication was associated with lower likelihood of ARNI prescription at discharge (OR, 0.11 [95% CI, 0.10-0.12]; P<0.001). Socioeconomic factors associated with lower likelihood of ARNI prescription included having no insurance (OR, 0.60 [95% CI, 0.50-0.72]; P<0.001) and living in a ZIP Code identified as distressed (OR, 0.81 [95% CI, 0.70-0.93]; P=0.010). The rate of ARNI prescription is increasing with time (OR, 2 [95% CI, 1.8-2.3]; P<0.001 for patients discharged in 2020 as opposed to 2017), but the disparity in prescription rates between distressed and prosperous communities appears to be increasing.
Conclusions: Multiple medical and socioeconomic factors contribute to low rates of ARNI prescription at hospital discharge. Potential targets for improving ARNI prescription rates include initiating ARNIs during hospitalization and aggressively addressing patients' access barriers with the support of inpatient social services and pharmacists.
Keywords: heart failure; neprilysin; odds ratio; practice patterns, physicians; socioeconomic factors.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757 - DOI - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–619. doi: 10.1161/HHF.0b013e318291329a - DOI - PMC - PubMed
-
- Writing Committee M, Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Colvin MM, Drazner MH, Filippatos G, Fonarow GC, et al. 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2016;134:e282–293. doi: 10.1161/CIR.0000000000000435 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
