

Respective Effects of Helmet Pressure Support, Continuous Positive Airway Pressure, and Nasal High-Flow in Hypoxemic Respiratory Failure: A Randomized Crossover Clinical Trial
- PMID: 36378814
- PMCID: PMC10595442
- DOI: 10.1164/rccm.202204-0629OC
Respective Effects of Helmet Pressure Support, Continuous Positive Airway Pressure, and Nasal High-Flow in Hypoxemic Respiratory Failure: A Randomized Crossover Clinical Trial
Erratum in
-
Erratum: Respective Effects of Helmet Pressure Support, Continuous Positive Airway Pressure, and Nasal High-Flow in Hypoxemic Respiratory Failure: A Randomized Crossover Clinical Trial.Am J Respir Crit Care Med. 2023 Nov 1;208(9):1004. doi: 10.1164/rccm.v208erratum3. Am J Respir Crit Care Med. 2023. PMID: 37909763 Free PMC article. No abstract available.
Abstract
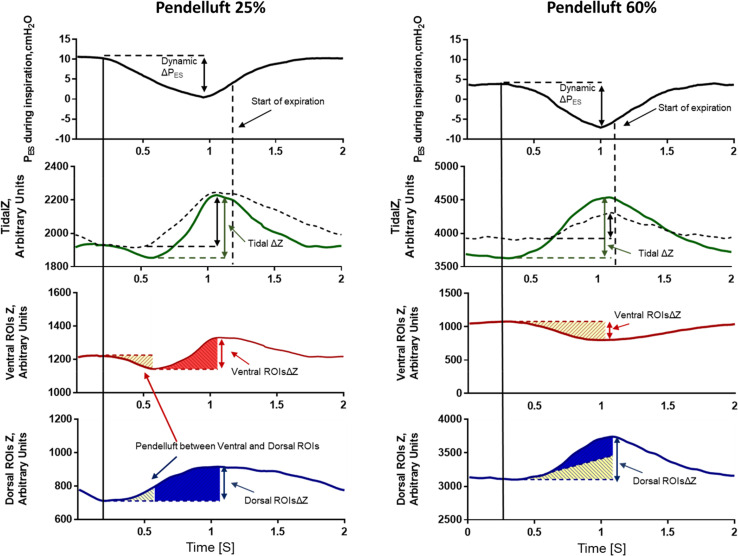
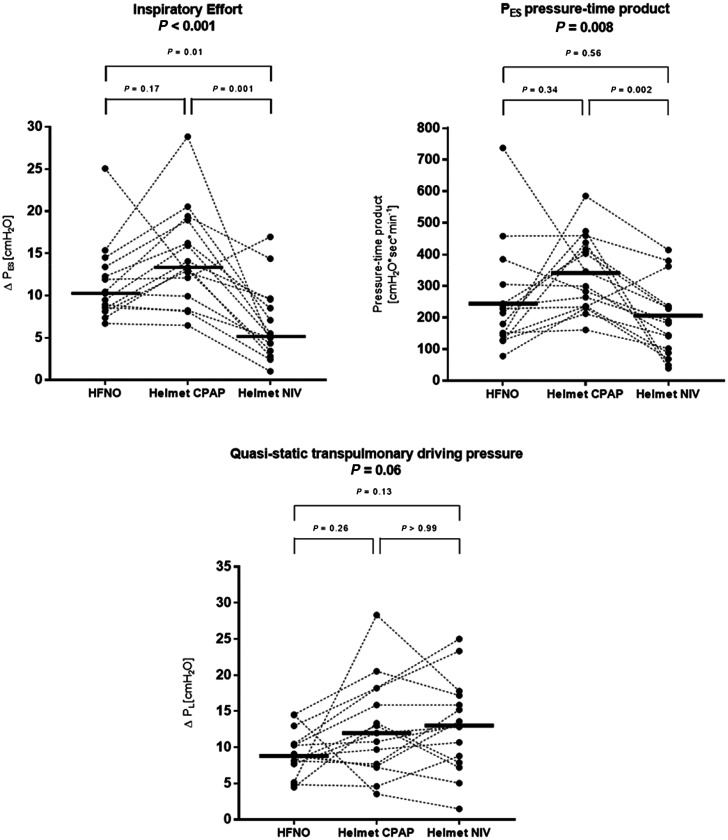
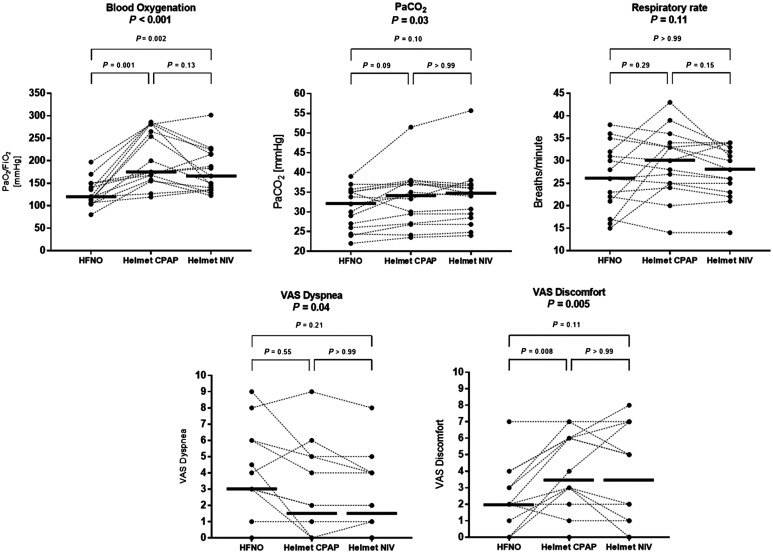
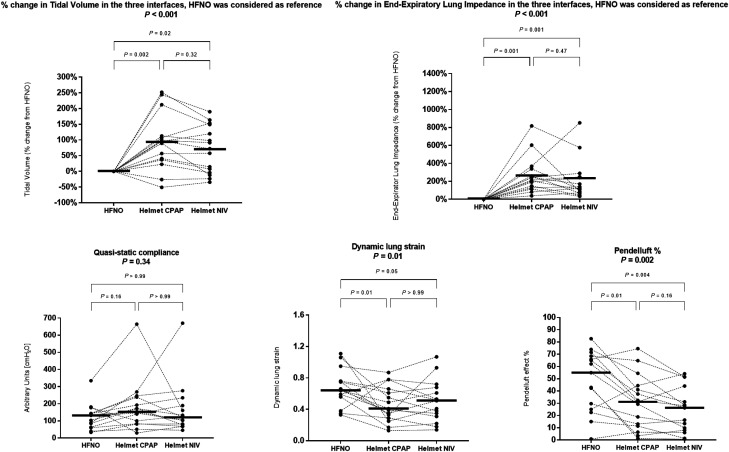
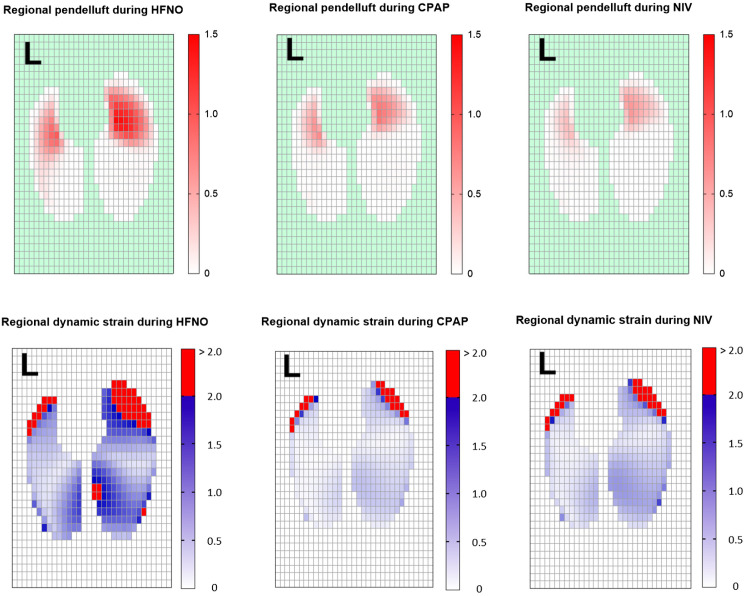
Rationale: The respective effects of positive end-expiratory pressure (PEEP) and pressure support delivered through the helmet interface in patients with hypoxemia need to be better understood. Objectives: To assess the respective effects of helmet pressure support (noninvasive ventilation [NIV]) and continuous positive airway pressure (CPAP) compared with high-flow nasal oxygen (HFNO) on effort to breathe, lung inflation, and gas exchange in patients with hypoxemia (PaO2/FiO2 ⩽ 200). Methods: Fifteen patients underwent 1-hour phases (constant FiO2) of HFNO (60 L/min), helmet NIV (PEEP = 14 cm H2O, pressure support = 12 cm H2O), and CPAP (PEEP = 14 cm H2O) in randomized sequence. Measurements and Main Results: Inspiratory esophageal (ΔPES) and transpulmonary pressure (ΔPL) swings were used as surrogates for inspiratory effort and lung distension, respectively. Tidal Volume (Vt) and end-expiratory lung volume were assessed with electrical impedance tomography. ΔPES was lower during NIV versus CPAP and HFNO (median [interquartile range], 5 [3-9] cm H2O vs. 13 [10-19] cm H2O vs. 10 [8-13] cm H2O; P = 0.001 and P = 0.01). ΔPL was not statistically different between treatments. PaO2/FiO2 ratio was significantly higher during NIV and CPAP versus HFNO (166 [136-215] and 175 [158-281] vs. 120 [107-149]; P = 0.002 and P = 0.001). NIV and CPAP similarly increased Vt versus HFNO (mean change, 70% [95% confidence interval (CI), 17-122%], P = 0.02; 93% [95% CI, 30-155%], P = 0.002) and end-expiratory lung volume (mean change, 198% [95% CI, 67-330%], P = 0.001; 263% [95% CI, 121-407%], P = 0.001), mostly due to increased aeration/ventilation in dorsal lung regions. During HFNO, 14 of 15 patients had pendelluft involving >10% of Vt; pendelluft was mitigated by CPAP and further by NIV. Conclusions: Compared with HFNO, helmet NIV, but not CPAP, reduced ΔPES. CPAP and NIV similarly increased oxygenation, end-expiratory lung volume, and Vt, without affecting ΔPL. NIV, and to a lesser extent CPAP, mitigated pendelluft. Clinical trial registered with clinicaltrials.gov (NCT04241861).
Keywords: acute hypoxemic respiratory failure; acute respiratory distress syndrome; helmet support; noninvasive ventilation.
Figures
Comment in
-
Enhancing Our Understanding of Breathing Mechanics in Nonintubated Patients with Acute Hypoxemic Respiratory Failure.Am J Respir Crit Care Med. 2023 May 15;207(10):1259-1260. doi: 10.1164/rccm.202212-2190ED. Am J Respir Crit Care Med. 2023. PMID: 36476173 Free PMC article. No abstract available.
-
The Proper Assessment of Pendelluft and Absolute End-Expiratory Lung Volume.Am J Respir Crit Care Med. 2023 Nov 1;208(9):1001-1002. doi: 10.1164/rccm.202306-1058LE. Am J Respir Crit Care Med. 2023. PMID: 37586081 Free PMC article. No abstract available.
References
-
- Oczkowski S, Ergan B, Bos L, Chatwin M, Ferrer M, Gregoretti C, et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J . 2022;59:2101574. - PubMed
-
- Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med . 2017;195:438–442. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
