

Immune biomarkers of response to immunotherapy in patients with high-risk smoldering myeloma
- PMID: 36379208
- PMCID: PMC10019228
- DOI: 10.1016/j.ccell.2022.10.017
Immune biomarkers of response to immunotherapy in patients with high-risk smoldering myeloma
Abstract
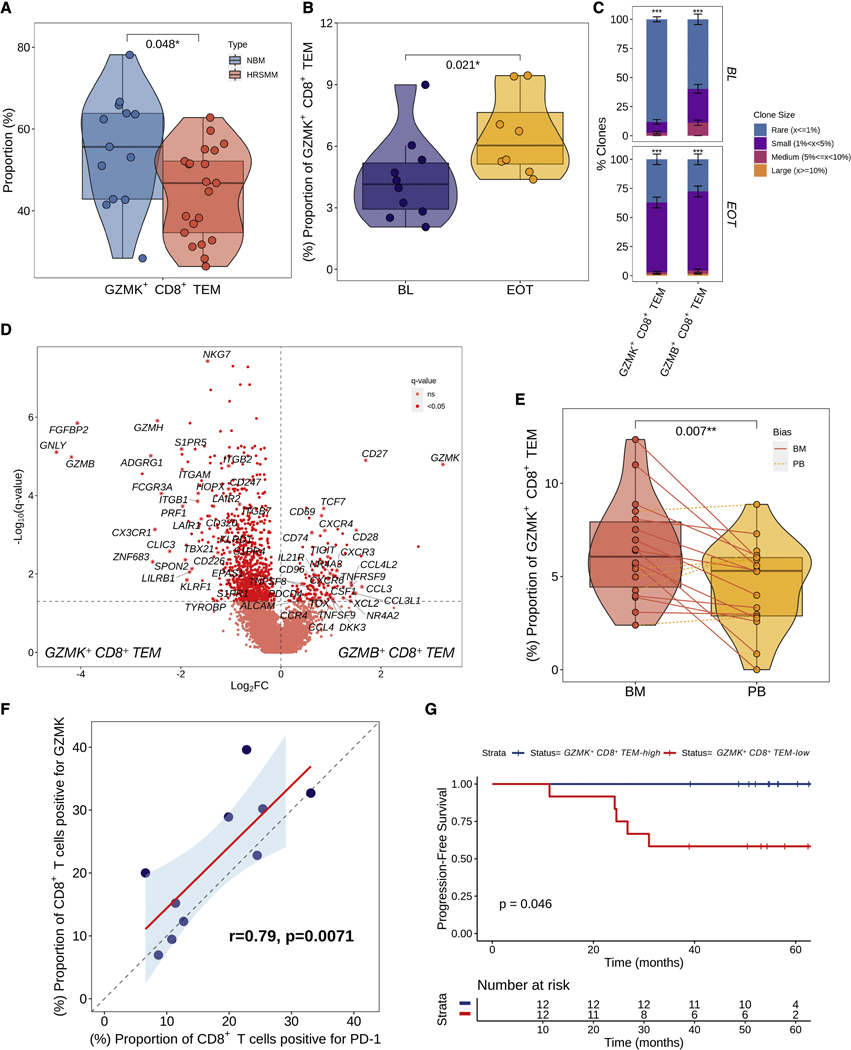
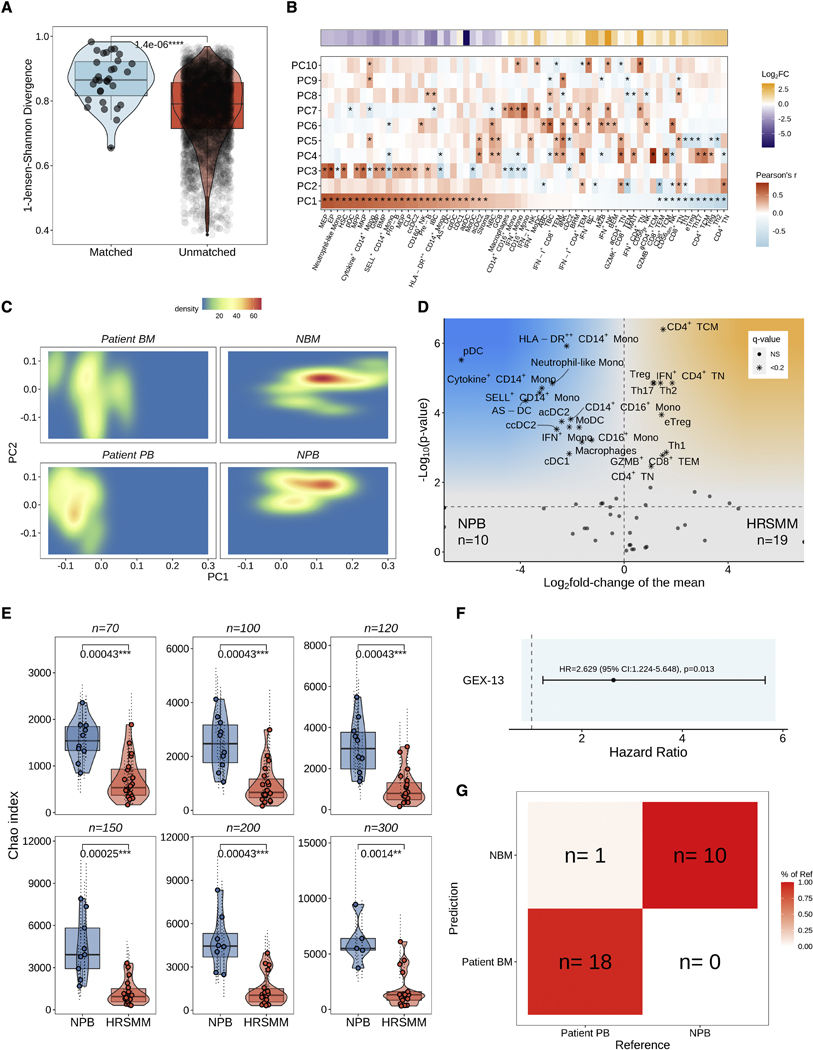
Patients with smoldering multiple myeloma (SMM) are observed until progression, but early treatment may improve outcomes. We conducted a phase II trial of elotuzumab, lenalidomide, and dexamethasone (EloLenDex) in patients with high-risk SMM and performed single-cell RNA and T cell receptor (TCR) sequencing on 149 bone marrow (BM) and peripheral blood (PB) samples from patients and healthy donors (HDs). We find that early treatment with EloLenDex is safe and effective and provide a comprehensive characterization of alterations in immune cell composition and TCR repertoire diversity in patients. We show that the similarity of a patient's immune cell composition to that of HDs may have prognostic relevance at diagnosis and after treatment and that the abundance of granzyme K (GZMK)+ CD8+ effector memory T (TEM) cells may be associated with treatment response. Last, we uncover similarities between immune alterations observed in the BM and PB, suggesting that PB-based immune profiling may have diagnostic and prognostic utility.
Keywords: bone marrow; granzyme K; immune biomarkers; immune profiling; immunotherapy; peripheral blood; single-cell RNA sequencing; single-cell TCR sequencing; smoldering multiple myeloma.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests N.J.H. is a consultant for Constellation Pharmaceuticals. F.A. is an employee of Illumina Inc. O.Z. is an employee of Ikena Oncology and a stockholder in Ikena Oncology and Morphosys AG. G.G. receives research funds from IBM and Pharmacyclics and is an inventor on patent applications filed by the Broad Institute related to MSMuTect, MSMutSig, POLYSOLVER, SignatureAnalyzer-GPU, and MSIDetect. He is also a founder and consultant of and holds privately held equity in Scorpion Therapeutics. I.M.G. has a consulting or advisory role with AbbVie, Adaptive, Amgen, Aptitude Health, Bristol Myers Squibb, GlaxoSmithKline, Huron Consulting, Janssen, Menarini Silicon Biosystems, Oncopeptides, Pfizer, Sanofi, Sognef, Takeda, The Binding Site, and Window Therapeutics and has received speaker fees from Vor Biopharma and Veeva Systems, Inc., and her spouse is the CMO and equity holder of Disc Medicine. S.M. has a consulting role with Abbvie, Adaptive Biotechnology, Amgen, Celgene/BMS, GlaxoSmithKline, Janssen, Novartis, Oncopeptides, Regeneron, Roche, and Takeda and has received research funding from Abbvie, Adaptive Biotechnology, Amgen, Celgene/BMS, GlaxoSmithKline, Janssen, Novartis, Oncopeptides, Regeneron, Roche, and Takeda. A.J.Y. has a consulting role with Adaptive Biotechnologies, Amgen, BMS, Celgene, GSK, Janssen, Karyopharm, Oncopeptides, Sanofi, and Takeda and has received research funding from Amgen, Janssen, and Takeda. M.B. is a consultant for Sanofi, Genzyme, and Janssen and has received research funding from MedImmune, Janssen, Legend Biotech, Amgen, Celularity, Bristol Myers Squibb, Celgene, Bluebird bio, Millennium, Takeda, Cerecor (currently Avalo Therapeutics), and C4 Therapeutics. M.B has an advisory role and received honoraria from Bristol Myers Squibb, Takeda, Janssen, and Menarini. T.H.M. received advisory board fees from Legend Biotech. R.S.-P., G.G., and I.M.G. are co-inventors on a patent application related to this work (PCT/US22/74839).
Figures
Comment in
-
Are we ready to look beyond plasma cells in assessing high-risk smoldering myeloma?Cancer Cell. 2022 Nov 14;40(11):1270-1272. doi: 10.1016/j.ccell.2022.10.014. Cancer Cell. 2022. PMID: 36379204
References
-
- Mateos MV, Kumar S, Dimopoulos MA, Gonzalez-Calle V, Kastritis E, Hajek R, De Larrea CF, Morgan GJ, Merlini G, Goldschmidt H, et al. (2020). International Myeloma Working Group risk stratification model for smoldering multiple myeloma (SMM). Blood Cancer J 10, 102. 10.1038/s41408-020-00366-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
