

This is a preprint.
Attenuated humoral responses in HIV infection after SARS-CoV-2 vaccination are linked to global B cell defects and cellular immune profiles
- PMID: 36380764
- PMCID: PMC9665338
- DOI: 10.1101/2022.11.11.516111
Attenuated humoral responses in HIV infection after SARS-CoV-2 vaccination are linked to global B cell defects and cellular immune profiles
Update in
-
Attenuated humoral responses in HIV after SARS-CoV-2 vaccination linked to B cell defects and altered immune profiles.iScience. 2023 Jan 20;26(1):105862. doi: 10.1016/j.isci.2022.105862. Epub 2022 Dec 24. iScience. 2023. PMID: 36590902 Free PMC article.
Abstract
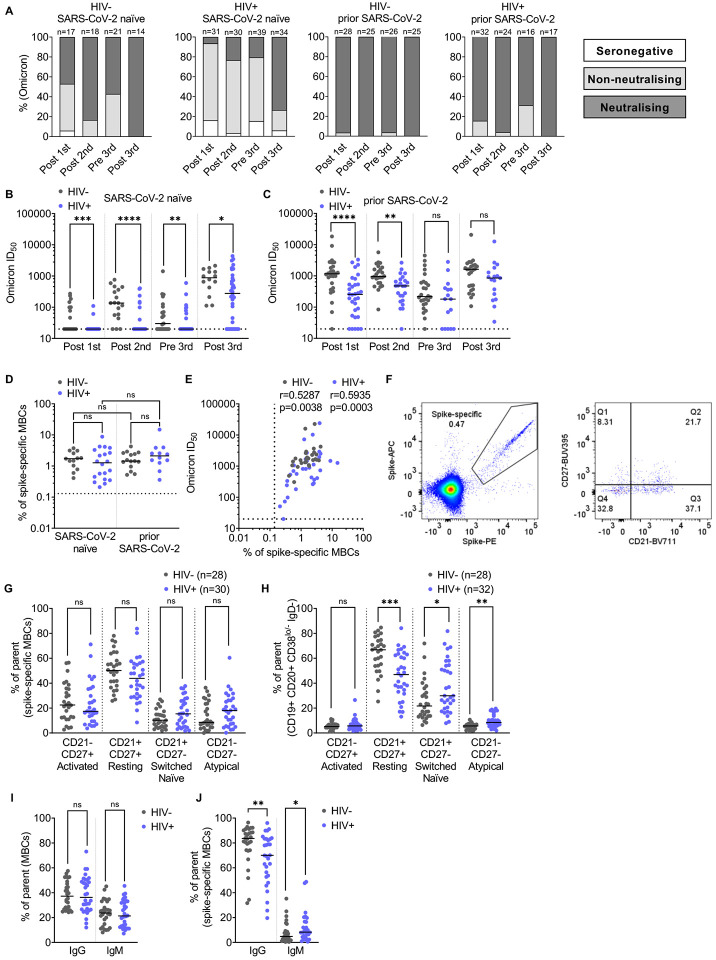
People living with HIV (PLWH) on suppressive antiretroviral therapy (ART) can have residual immune dysfunction and often display poorer responses to vaccination. We assessed in a cohort of PLWH (n=110) and HIV negative controls (n=64) the humoral and spike-specific B-cell responses following 1, 2 or 3 SARS-CoV-2 vaccine doses. PLWH had significantly lower neutralizing antibody (nAb) titers than HIV-negative controls at all studied timepoints. Moreover, their neutralization breadth was reduced with fewer individuals developing a neutralizing response against the Omicron variant (BA.1) relative to controls. We also observed a delayed development of neutralization in PLWH that was underpinned by a reduced frequency of spike-specific memory B cells (MBCs) and pronounced B cell dysfunction. Improved neutralization breadth was seen after the third vaccine dose in PLWH but lower nAb responses persisted and were associated with global, but not spike-specific, MBC dysfunction. In contrast to the inferior antibody responses, SARS-CoV-2 vaccination induced robust T cell responses that cross-recognized variants in PLWH. Strikingly, a subset of PLWH with low or absent neutralization had detectable functional T cell responses. These individuals had reduced numbers of circulating T follicular helper cells and an enriched population of CXCR3 + CD127 + CD8 + T cells after two doses of SARS-CoV-2 vaccination, which may compensate for sub-optimal serological responses in the event of infection. Therefore, normalisation of B cell homeostasis could improve serological responses to vaccines in PLWH and evaluating T cell immunity could provide a more comprehensive immune status profile in these individuals and others with B cell imbalances.
Figures





References
-
- Banki Z., Mateus J., Rossler A., Schafer H., Bante D., Riepler L., Grifoni A., Sette A., Simon V., Falkensammer B., et al. (2022). Heterologous ChAdOx1/BNT162b2 vaccination induces stronger immune response than homologous ChAdOx1 vaccination: The pragmatic, multi-center, three-arm, partially randomized HEVACC trial. EBioMedicine 80, 104073. - PMC - PubMed
-
- Bergamaschi L., Mescia F., Turner L., Hanson A.L., Kotagiri P., Dunmore B.J., Ruffieux H., De Sa A., Huhn O., Morgan M.D., et al. (2021). Longitudinal analysis reveals that delayed bystander CD8+ T cell activation and early immune pathology distinguish severe COVID-19 from mild disease. Immunity 54, 1257–1275 e1258. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous