

Definition of clinically insignificant residual fragments after percutaneous nephrolithotomy among urologists: a world-wide survey by EAU-YAU Endourology and Urolithiasis Working Group
- PMID: 36381161
- PMCID: PMC9628728
- DOI: 10.5173/ceju.2022.0115
Definition of clinically insignificant residual fragments after percutaneous nephrolithotomy among urologists: a world-wide survey by EAU-YAU Endourology and Urolithiasis Working Group
Abstract
Introduction: The aim of this article was to evaluate the current perception of urologists as to what size is considered as a clinically insignificant residual fragment (CIRF).
Material and methods: A survey was globally distributed to the members of the Endourological Society via SurveyMonkey.
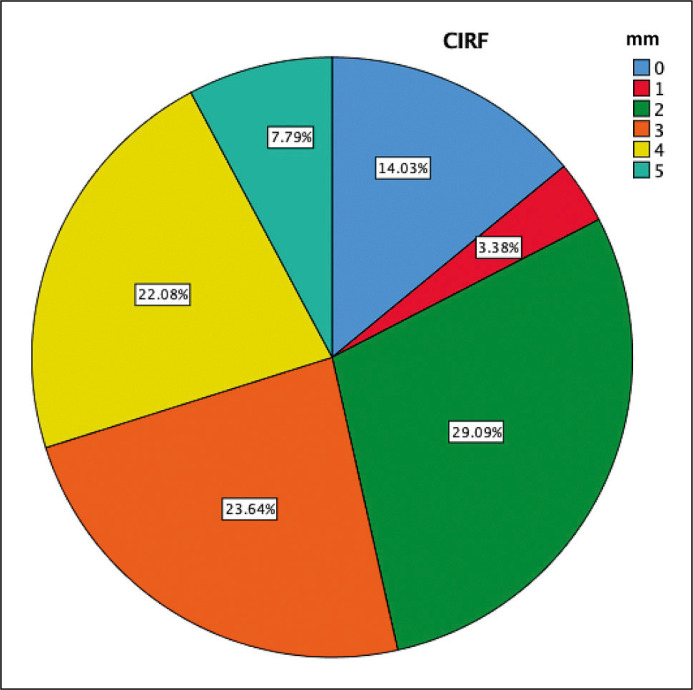
Results: A total of 385 participants responded to the survey on CIRF. Most participants considered 2 mm (29%) as CIRF threshold, followed by 3 mm (24%), 4 mm (22%), 0 mm (14%), 5 mm (8%) and 1 mm (3%). North American urologists considered CIRF to be smaller than urologists from Asia, Eurasia and South America, (p-values ≤0.001, 0.037 and 0.015 respectively). European urologists identified smaller CIRF in comparison to Asian urologists (p-value = 0.001). Urologists mainly using a pneumatic lithotripter accepted larger fragments as CIRF, compared to urologists mainly using ultrasonic devices or a combination of ultrasonic and pneumatic devices (p-value = 0.026 and 0.005 respectively). Similarly, urologists mainly performing X-Ray and ultrasound as post-operative imaging accepted larger fragments as CIRF in comparison to urologists mainly performing non-contrast computed tomography (p-value = 0.001).
Conclusions: What is considered as CIRF varies between urologist from different continents and seems to be associated with the lithotripter used and the post-operative imaging modality of preference to assess treatment success.
Keywords: clinically insignificant residual fragment; imaging; percutaneous nephrolithotomy; survey.
Copyright by Polish Urological Association.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Bartoletti R, Cai T, Mondaini N, Melone F, Travaglini F, Carini M, Rizzo M. Epidemiology and risk factors in urolithiasis. Urol Int. 2007; 79 (Suppl 1): 3-7. - PubMed
-
- Wang YB, Cui YX, Song JN, Yang Q, Wang G. Efficacies of various surgical regimens in the treatment of renal calculi patients: a network meta-analysis in 25 enrolled controlled clinical trials. Kidney Blood Press Res. 2018; 43: 1183-1198. - PubMed
-
- Suarez-Ibarrola R, Hein S, Miernik A. Residual stone fragments: clinical implications and technological innovations. Curr Opin Urol. 2019; 29: 129-134. - PubMed
-
- Opondo D, Gravas S, Joyce A, et al. . Standardization of patient outcomes reporting in percutaneous nephrolithotomy. J Endourol. 2014; 28: 767-774. - PubMed
-
- Kulb TB, Lingeman JE, Coury TA, et al. . Extracorporeal Shock Wave Lithotripsy in Patients with a Solitary Kidney. J Urol. 1986; 136: 786-788. - PubMed
LinkOut - more resources
Full Text Sources