

State-of-the-art management of dysplastic Barrett's esophagus
- PMID: 36381221
- PMCID: PMC9651477
- DOI: 10.1093/gastro/goac068
State-of-the-art management of dysplastic Barrett's esophagus
Abstract
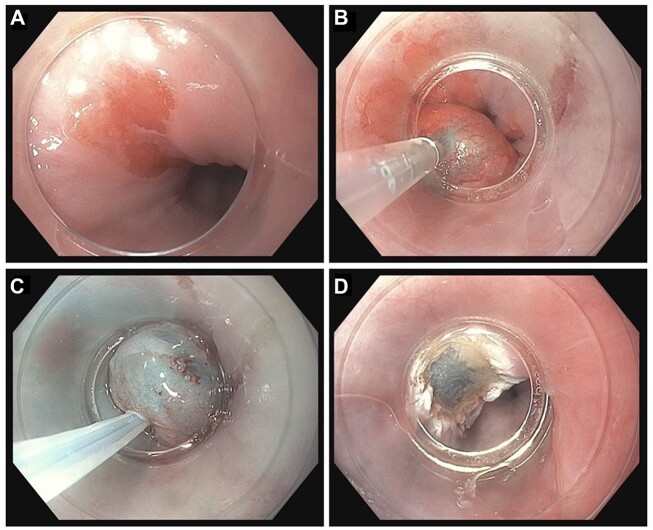
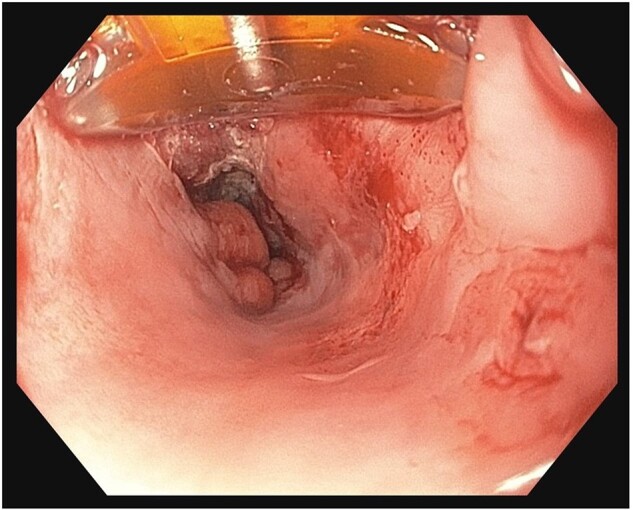
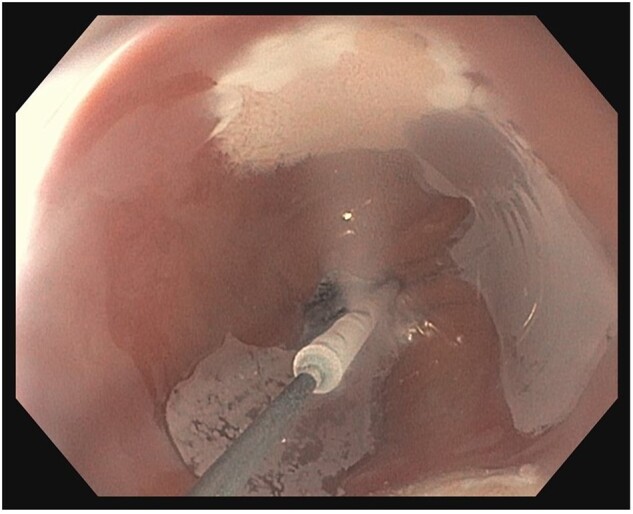
Endoscopic eradication therapy (EET) has become a standard of care for treatment of dysplastic Barrett's esophagus (BE) and early Barrett's neoplasia. EET mainly consists of removal of any visible lesions via endoscopic resection and eradication of all remaining Barrett's mucosa using endoscopic ablation. Endoscopic mucosal resection and endoscopic submucosal dissection are the two available resection techniques. After complete resection of all visible lesions, it is crucial to perform endoscopic ablation to ensure complete eradication of the remaining Barrett's segment. Endoscopic ablation can be done either with thermal techniques, including radiofrequency ablation and argon plasma coagulation, or cryotherapy techniques. The primary end point of EET is achieving complete remission of intestinal metaplasia (CRIM) to decrease the risk of dysplastic recurrence after successful EET. After CRIM is achieved, a standardized endoscopic surveillance protocol needs to be implemented for early detection of BE recurrence.
Keywords: Barrett’s esophagus; endoscopic eradication therapy; endoscopic mucosal resection; endoscopic submucosal dissection; esophageal adenocarcinoma.
© The Author(s) 2022. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Figures



References
-
- Singh S, Manickam P, Amin AV. et al. Incidence of esophageal adenocarcinoma in Barrett's esophagus with low-grade dysplasia: a systematic review and meta-analysis. Gastrointest Endosc 2014;79:897–909.e4. quiz 83.e1–e3. - PubMed
-
- Rastogi A, Puli S, El-Serag HB. et al. Incidence of esophageal adenocarcinoma in patients with Barrett's esophagus and high-grade dysplasia: a meta-analysis. Gastrointest Endosc 2008;67:394–8. - PubMed
-
- American Gastroenterological A, Spechler SJ, Sharma P. et al.; American Gastroenterological Association. American Gastroenterological Association medical position statement on the management of Barrett's esophagus. Gastroenterology 2011;140:1084–91. - PubMed
-
- Phoa KN, van Vilsteren FG, Weusten BL. et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial. JAMA 2014;311:1209–17. - PubMed
-
- Shaheen NJ, Sharma P, Overholt BF. et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med 2009;360:2277–88. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
