

World Heart Federation Cholesterol Roadmap 2022
- PMID: 36382159
- PMCID: PMC9562775
- DOI: 10.5334/gh.1154
World Heart Federation Cholesterol Roadmap 2022
Abstract
Background: Atherosclerotic cardiovascular diseases (ASCVD) including myocardial infarction, stroke and peripheral arterial disease continue to be major causes of premature death, disability and healthcare expenditure globally. Preventing the accumulation of cholesterol-containing atherogenic lipoproteins in the vessel wall is central to any healthcare strategy to prevent ASCVD. Advances in current concepts about reducing cumulative exposure to apolipoprotein B (apo B) cholesterol-containing lipoproteins and the emergence of novel therapies provide new opportunities to better prevent ASCVD. The present update of the World Heart Federation Cholesterol Roadmap provides a conceptual framework for the development of national policies and health systems approaches, so that potential roadblocks to cholesterol management and thus ASCVD prevention can be overcome.
Methods: Through a review of published guidelines and research papers since 2017, and consultation with a committee composed of experts in clinical management of dyslipidaemias and health systems research in low-and-middle income countries (LMICs), this Roadmap identifies (1) key principles to effective ASCVD prevention (2) gaps in implementation of these interventions (knowledge-practice gaps); (3) health system roadblocks to treatment of elevated cholesterol in LMICs; and (4) potential strategies for overcoming these.
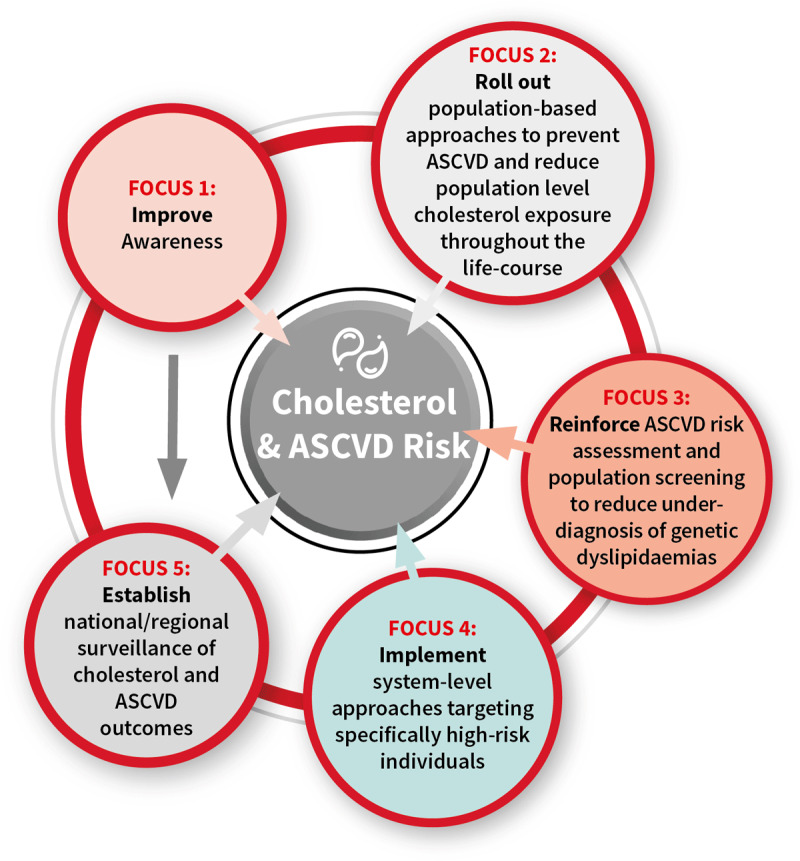
Results: Reducing the future burden of ASCVD will require diverse approaches throughout the life-course. These include: a greater focus on primordial prevention; availability of affordable cholesterol testing; availability of universal cholesterol screening for inherited dyslipidaemias; risk stratification moving beyond 10-year risk to look at lifetime risk with adequate risk estimators; wider availability of affordable cholesterol-lowering therapies which should include statins as essential medications globally; use of adequate doses of potent statin regimens; and combination therapies with ezetimibe or other therapies in order to attain and maintain robust reductions in LDL-C in those at highest risk. Continuing efforts are needed on health literacy for both the public and healthcare providers, utilising multi-disciplinary teams in healthcare and applications that quantify both ASCVD risk and benefits of treatment as well as increased adherence to therapies.
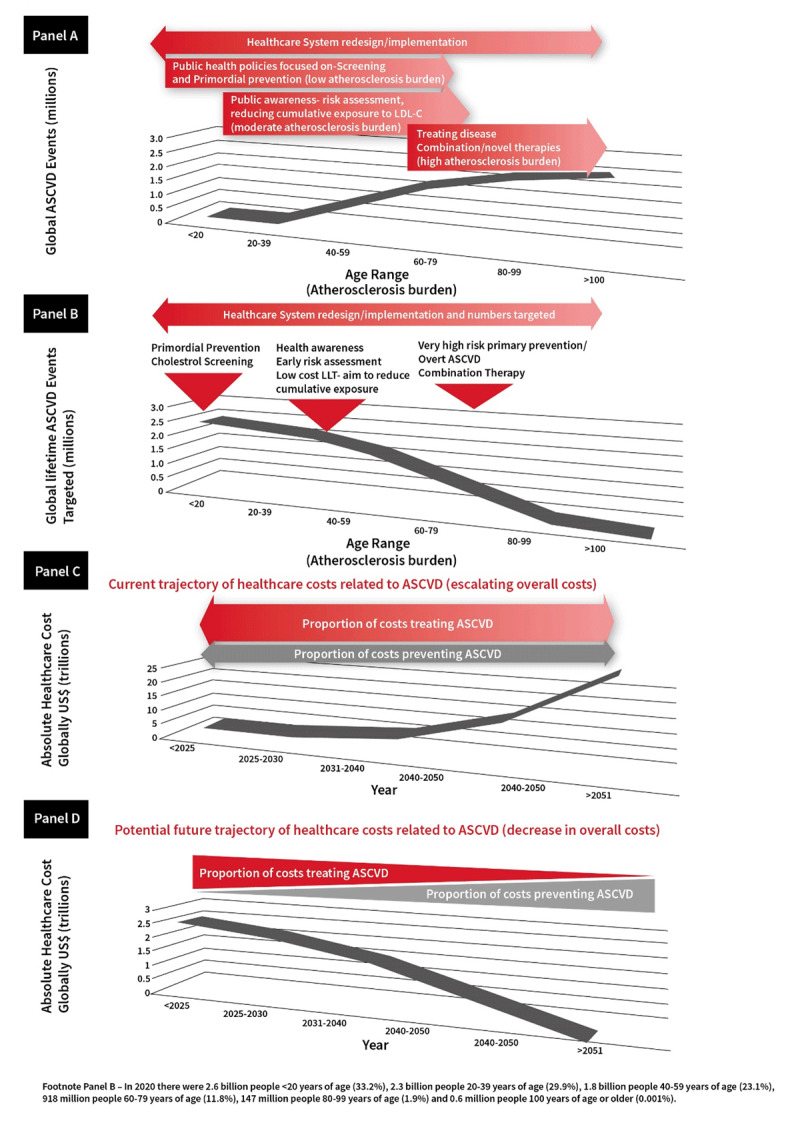
Conclusions: The adverse effects of LDL-cholesterol and apo B containing lipoprotein exposure are cumulative and result in ASCVD. These are preventable by implementation of different strategies, aimed at efficiently tackling atherosclerosis at different stages throughout the human life-course. Preventive strategies should therefore be updated to implement health policy, lifestyle changes and when needed pharmacotherapies earlier with investment in, and a shift in focus towards, early preventive strategies that preserve cardiovascular health rather than treat the consequences of ASCVD.
Keywords: ASCVD; cholesterol; familial hypercholesterolaemia; lipid lowering therapy; low-density lipoprotein cholesterol prevention.
Copyright: © 2022 The Author(s).
Conflict of interest statement
Kausik K. Ray has received honoraria for consulting, lectures from Kowa, Amgen, Regeneron Pharmaceuticals, Sanofi, Daiichi Sankyo, Pfizer, Viatris, AstraZeneca, Eli Lilly, Esperion, New Amsterdam Pharma, Novartis, Silence Therapeutics, Bayer, Boehringer Ingelheim, Novo Nordisk, SCRIBE, CRISPR, Cargene, Vaxxinity, Abbott, Resverlogix. In addition, he has received research grant support to his institution from Sanofi, Daiichi Sankyo, Amgen, Pfizer and MSD and support from the NIHR Imperial Biomedical Research Centre. Brian A. Ference has received research grants from Novartis, Amgen, Pfizer, Merck, and Esperion Therapeutics. In addition, the author has received personal fees for consulting, advisory board participation and lectures from Novartis, Amgen, Regeneron, Sanofi, Merck, Pfizer, Eli Lilly, Novo Nordisk, AstraZeneca, Viatris, The Medicines Co, Mylan, Daiichi Sankyo, dalCOR, CiVi Pharma, KrKa Phamaceuticals, the American College of Cardiology, the European Society of Cardiology, and the European Atherosclerosis Society. Dirk J. Blom has received research grants from Amgen, Amryt, AstraZeneca, IONIS, LIB Therapeutics, Novartis, Regeneron, Sanofi; Lecture fees and personal fees from Amgen, Novartis, Organon, Sandoz, Sanofi and has participated in advisory board for Amgen, Amryt (Chair of the LOWER study steering committee), and Sanofi. Stephen J. Nicolls has benefitted from research support from AstraZeneca, New Amsterdam Pharma, Amgen, Anthera, Eli Lilly, Esperion, Novartis, Cerenis, The Medicines Company, Resverlogix, InfraReDx, Roche, Sanofi-Regeneron and LipoScience and consulting and honoraria fees from AstraZeneca, Amarin, Akcea, Eli Lilly, Anthera, Omthera, Merck, Takeda, Resverlogix, Sanofi-Regeneron, CSL Behring, Esperion, Boehringer Ingelheim, Sequirus. Rodrigo Alonso has received honorary fees and participation in pharma symposia or advisory boards in the last five years from Amgen, Tecnofarma, SAVAL, ABBOTT, NovoNordisk, Boehringer-Ingelheim and Teva. Piotr Jankowski has received Honoraria and travel grants from Amgen, Sanofi, Servier. Roopa Mehta has been part of the speakers’ bureau for Amgen. Nathan D. Wong has received Research support through his institution from Novartis and Novo Nordisk and has been a consultant to Novartis. As Co-Principal Investigator of INTERASPIRE, David A. Wood’s Institute is in receipt of Independent Investigator Initiated grants from Abbott, Novartis, Pfizer, Sanofi, Viatris. Samuel S. Gidding has been a consultant on paediatric clinical trials of bempedoic acid for Esperion. Fausto J. Pinto has participated in Advisory Board, Speaker’s bureau, and clinical trials with Astra-Zeneca, Daichii Sankyo, Amgen, Sanofi. Raul D. Santos has received honoraria related to speaker activities, consulting or research from: Abbott, Ache, Abbott, Amgen, Astra Zeneca, Biolab, EMS, Hypera, Libbs, Esperion, Kowa, Getz pharma, Novo-Nordisk, Novartis, Merck, PTC therapeutics, Pfizer, and Sanofi.
Figures
References
-
- Rittiphairoj T, Reilly A, Reddy CL, Barrenho E, Colombo FRA. The State of Cardiovascular Disease in G20+ countries. Health Systems Innovation Lab, Harvard University; 2022.
