

Stress fractures
- PMID: 36382766
- PMCID: PMC10118812
- DOI: 10.20945/2359-3997000000562
Stress fractures
Abstract
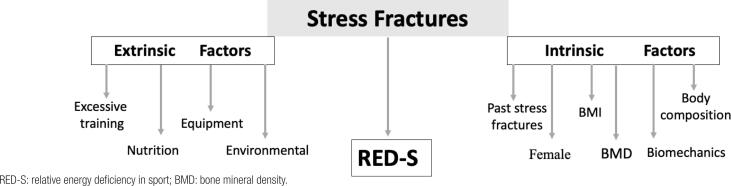
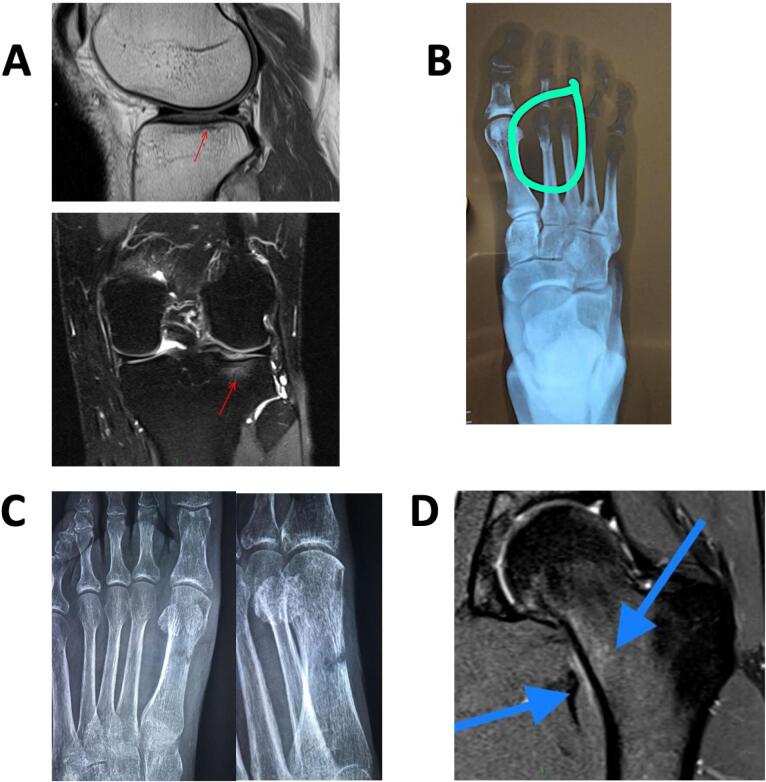
Stress fractures (SF) represent 10%-20% of all injuries in sport medicine. An SF occurs when abnormal and repetitive loading is applied on normal bone: The body cannot adapt quickly enough, leading to microdamage and fracture. The etiology is multifactorial with numerous risk factors involved. Diagnosis of SF can be achieved by identifying intrinsic and extrinsic factors, obtaining a good history, performing a physical exam, and ordering laboratory and imaging studies (magnetic resonance imaging is the current gold standard). Relative energy deficiency in sport (RED-S) is a known risk factor. In addition, for women, it is very important know the menstrual status to identify long periods of amenorrhea in the past and the present. Early detection is important to improve the chance of symptom resolution with conservative treatment. Common presentation involves complaints of localized pain, with or without swelling, and tenderness on palpation of bony structures that begins earlier in training and progressively worsens with activity over a 2- to 3-week period. Appropriate classification of SF based on type, location, grading, and low or high risk is critical in guiding treatment strategies and influencing the time to return to sport. Stress injuries at low-risk sites are typically managed conservatively. Studies have suggested that calcium and vitamin D supplementation might be helpful. Moreover, other treatment regimens are not well established. Understanding better the pathophysiology of SFs and the potential utility of current and future bone-active therapeutics may well yield approaches that could treat SFs more effectively.
Keywords: RED syndrome; Stress fractures; athlete triad; magnetic resonance; overtraining.
Conflict of interest statement
Disclosure: no potential conflict of interest relevant to this article was reported.
Figures
References
-
- Shapiro M, Zubkov K, Landau R. Diagnosis of Stress fractures in military trainees: a large-scale cohort. BMJ Mil Health. 2022 Oct;168(5):382–385. - PubMed
-
- Saunier J, Chapurlat R. Stress fracture in athletes. Joint Bone Spine. 2018;85(3):307–310. - PubMed
-
- Knapik J, Montain SJ, McGraw S, Grier T, Ely M, Jones BH. Stress fracture risk factors in basic combat training. Int J Sports Med. 2012;33(11):940–946. - PubMed
-
- Tenforde AS, Kraus E, Fredericson M. Bone Stress Injuries in Runners. Phys Med Rehabil Clin N Am. 2016;27(1):139–149. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous