

Visualization of exhaled breath metabolites reveals distinct diagnostic signatures for acute cardiorespiratory breathlessness
- PMID: 36383685
- PMCID: PMC7613858
- DOI: 10.1126/scitranslmed.abl5849
Visualization of exhaled breath metabolites reveals distinct diagnostic signatures for acute cardiorespiratory breathlessness
Abstract
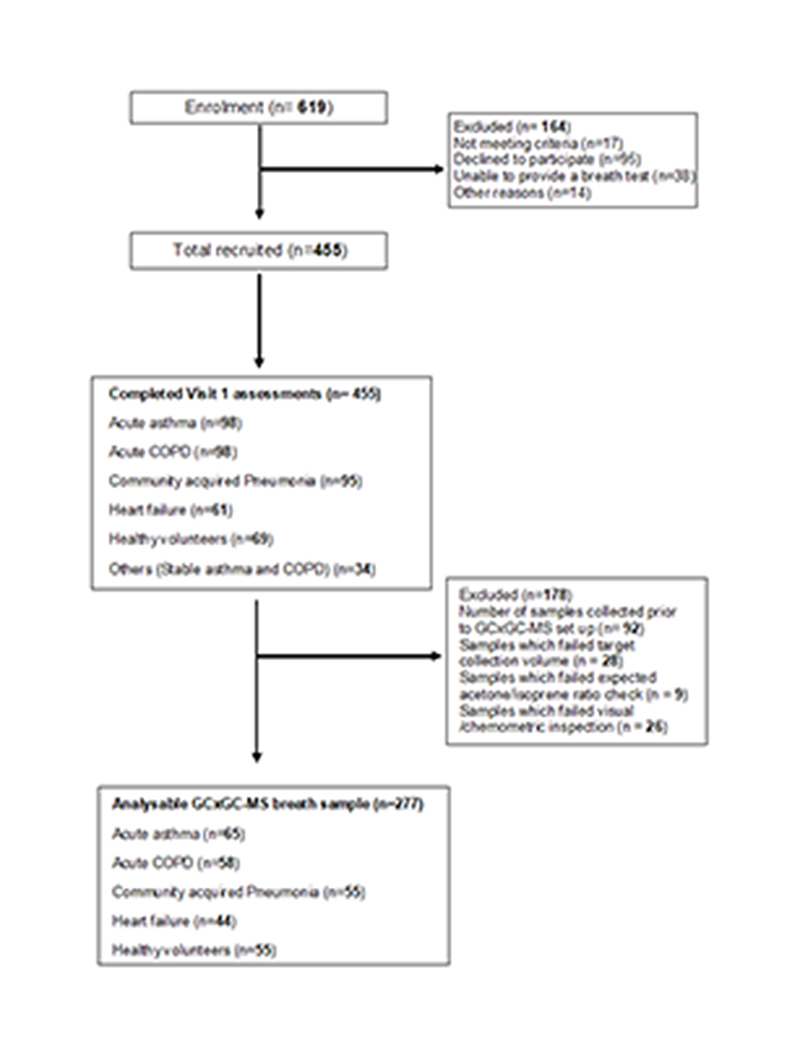
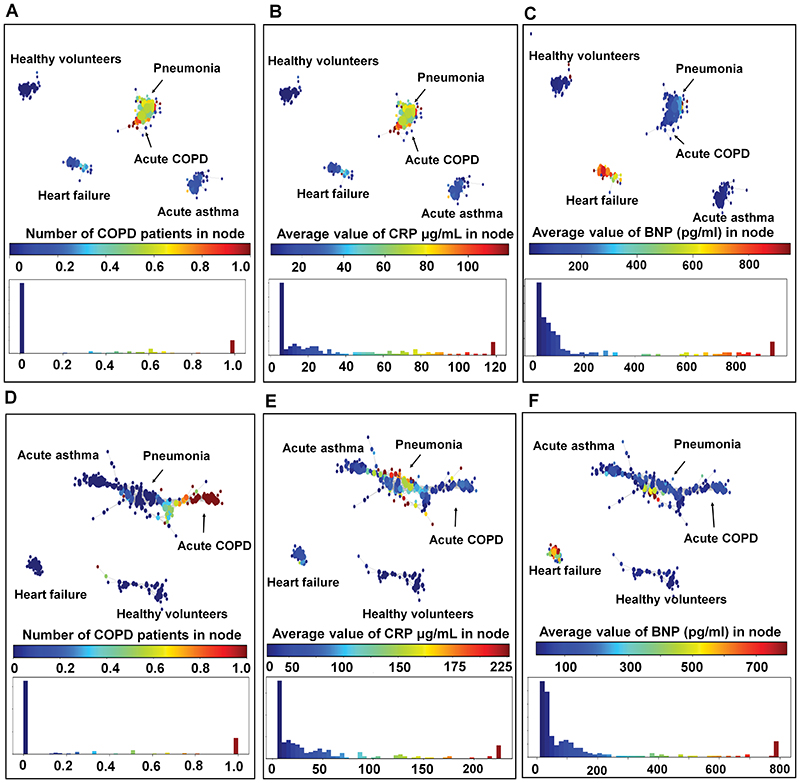
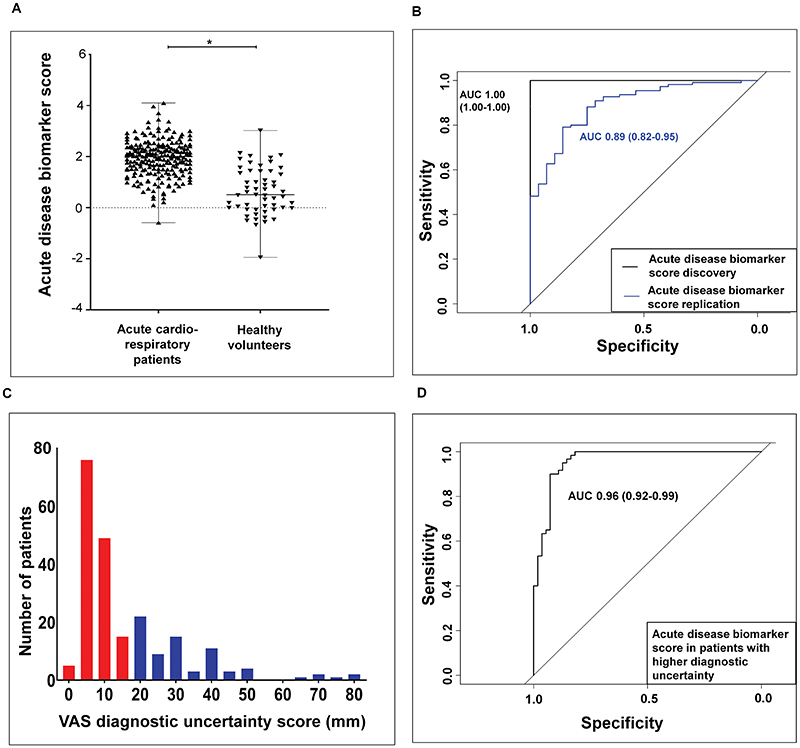
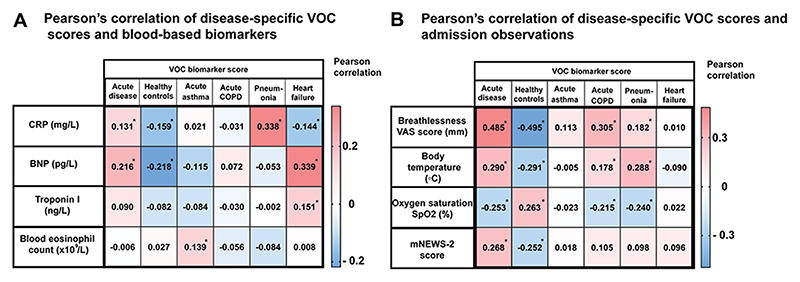
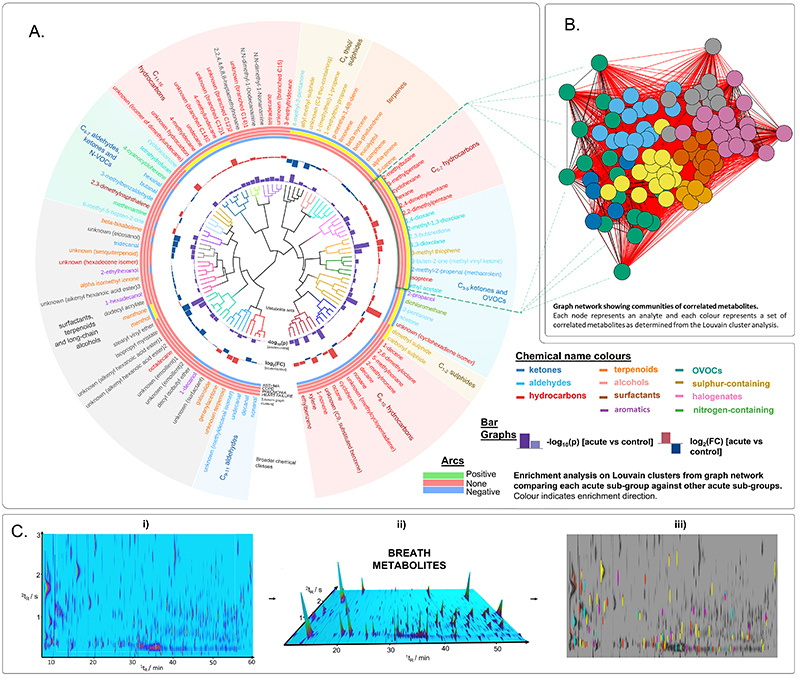
Acute cardiorespiratory breathlessness accounts for one in eight of all emergency hospitalizations. Early, noninvasive diagnostic testing is a clinical priority that allows rapid triage and treatment. Here, we sought to find and replicate diagnostic breath volatile organic compound (VOC) biomarkers of acute cardiorespiratory disease and understand breath metabolite network enrichment in acute disease, with a view to gaining mechanistic insight of breath biochemical derangements. We collected and analyzed exhaled breath samples from 277 participants presenting acute cardiorespiratory exacerbations and aged-matched healthy volunteers. Topological data analysis phenotypes differentiated acute disease from health and acute cardiorespiratory exacerbation subtypes (acute heart failure, acute asthma, acute chronic obstructive pulmonary disease, and community-acquired pneumonia). A multibiomarker score (101 breath biomarkers) demonstrated good diagnostic sensitivity and specificity (≥80%) in both discovery and replication sets and was associated with all-cause mortality at 2 years. In addition, VOC biomarker scores differentiated metabolic subgroups of cardiorespiratory exacerbation. Louvain clustering of VOCs coupled with metabolite enrichment and similarity assessment revealed highly specific enrichment patterns in all acute disease subgroups, for example, selective enrichment of correlated C5-7 hydrocarbons and C3-5 carbonyls in heart failure and selective depletion of correlated aldehydes in acute asthma. This study identified breath VOCs that differentiate acute cardiorespiratory exacerbations and associated subtypes and metabolic clusters of disease-associated VOCs.
Conflict of interest statement
C.E.B. has received consultancy and or grants paid to his Institution from GlaxoSmithKline (GSK), Astrazeneca (AZ), Boehringer Ingelheim (BI), Novartis, Chiesi,Genentech, Roche, Sanofi, Regeneron, TEVA Pharmaceuticals, MSD, Mologic, CSL Behring, Gossamer and 4Dpharma. SS has received funding from the MRC/EPSRC and University of Leicester for the research program presented in the manuscript. S.S. has engaged in consultancies/received speaker fees related to asthma, COPD, lung physiology and eosinophilic airway diseases from the following companies: Boehringer Ingelheim, Chiesi, Novartis, GSK, AZ, ERT Medical, Owlstone Medical, CSL Behring, Mundipharma, Knopp biotech. The rest of the co-authors have no competing interests to declare. E.G reports consultancy work for Boehringer Ingelheim with money paid to the institution (University of Leicester); Investigator led research grant from Circassia Group, Gilead Sciences, Chiesi Limited and Propeller Health; Research collaboration with Medimmune and Adherium (NZ) Limited; and speaker fees Circassia Group. The work presented in this paper has been filed by S.S, R.C, M.W, C.E.B, D.S, and P.T as part of UK Patent Application No. 2110365.0 and International Patent Application No. PCT/GB2022/051858.
Figures
References
-
- D. American Thoracic Society Committee on. Parshall MB, Schwartzstein RM, Adams L, Banzett RB, Manning HL, Bourbeau J, Calverley PM, Gift AG, Harver A, Lareau SC, et al. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. American journal of respiratory and critical care medicine. 2012;185:435–452. doi: 10.1164/rccm.201111-2042ST. - DOI - PMC - PubMed
-
- Schleich FN, Zanella D, Stefanuto PH, Bessonov K, Smolinska A, Dallinga JW, Henket M, Paulus V, Guissard F, Graff S, Moermans C, et al. Exhaled Volatile Organic Compounds are Able to Discriminate between Neutrophilic and Eosinophilic Asthma. Am J Respir Crit Care Med. 2019 doi: 10.1164/rccm.201811-2210OC. published online EpubApr 11. - DOI - PubMed
-
- Wilde MJ, Cordell RL, Salman D, Zhao B, Ibrahim W, Bryant L, Ruszkiewicz D, Singapuri A, Free RC, Gaillard EA, Beardsmore C, et al. Breath analysis by two-dimensional gas chromatography with dual flame ionisation and mass spectrometric detection - Method optimisation and integration within a large-scale clinical study. J Chromatogr A. 2019;1594:160–172. doi: 10.1016/j.chroma.2019.02.001. published online EpubJun 7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
