

Tools to Detect Risk of Death by Suicide: A Systematic Review and Meta-Analysis
- PMID: 36383739
- PMCID: PMC9890591
- DOI: 10.4088/JCP.21r14385
Tools to Detect Risk of Death by Suicide: A Systematic Review and Meta-Analysis
Abstract
Objective: There is limited knowledge about the ability of instruments to detect risk of suicide in a range of settings. Prior reviews have not considered whether the utility of instruments depends on prior probability of risk. We performed a systematic review to determine the diagnostic accuracy of instruments to detect risk of suicide in adults using likelihood ratio analysis. This method aids evaluation of prior probabilities of risk.
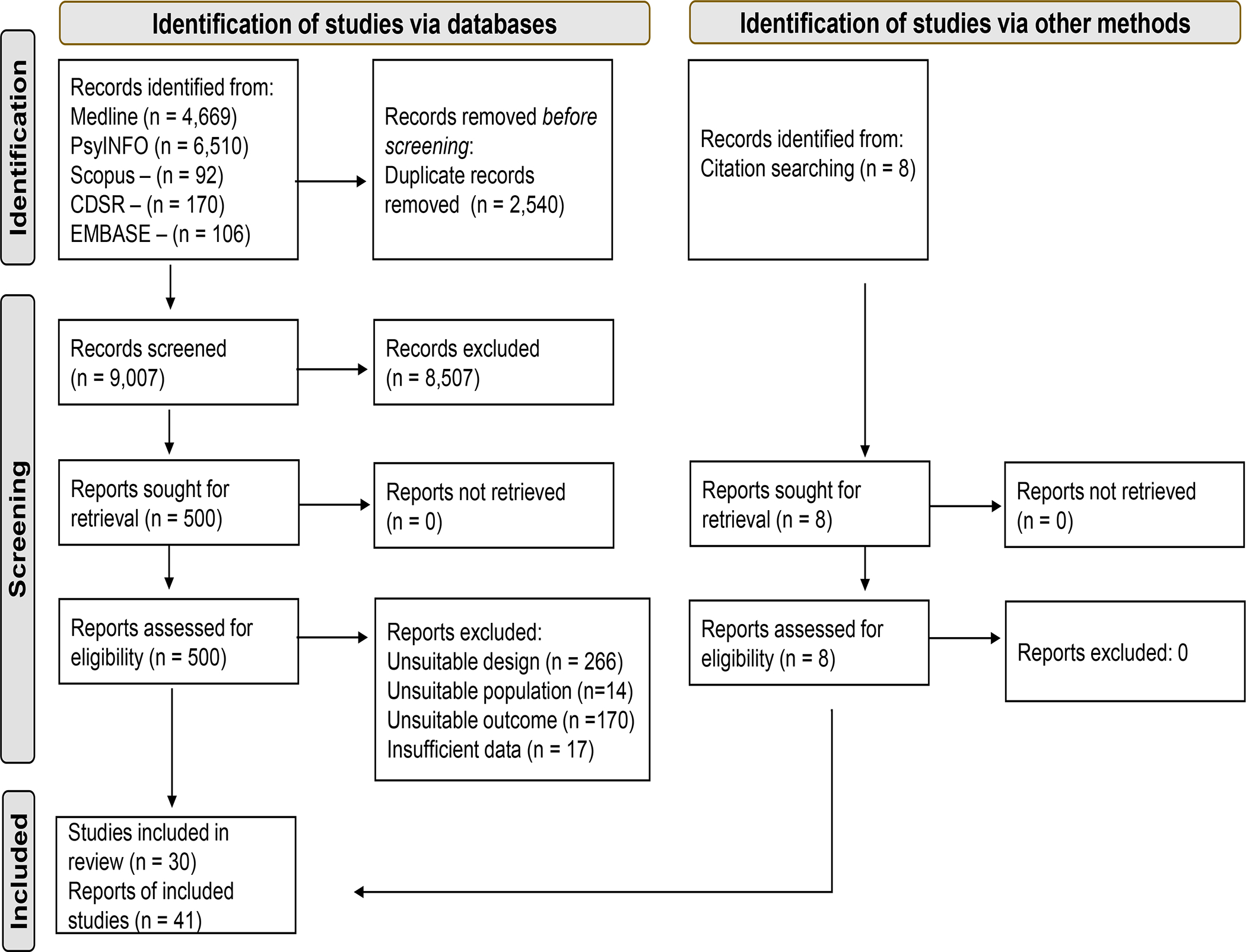
Data Sources: We searched MEDLINE, Cochrane Database of Systematic Reviews, PsycINFO, EMBASE, and Scopus from inception through January 19, 2021.
Study Selection: We included clinical trials, observational studies, and quasi-experimental studies assessing the diagnostic accuracy of instruments to detect risk of suicide in adults. There were no language restrictions.
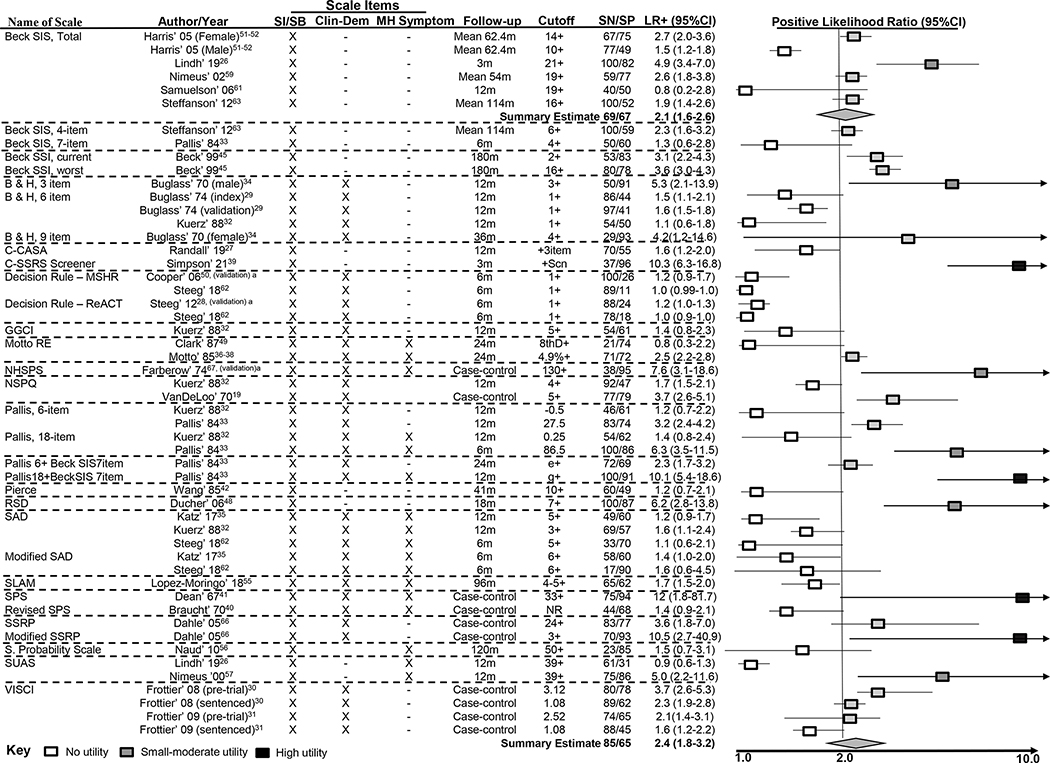
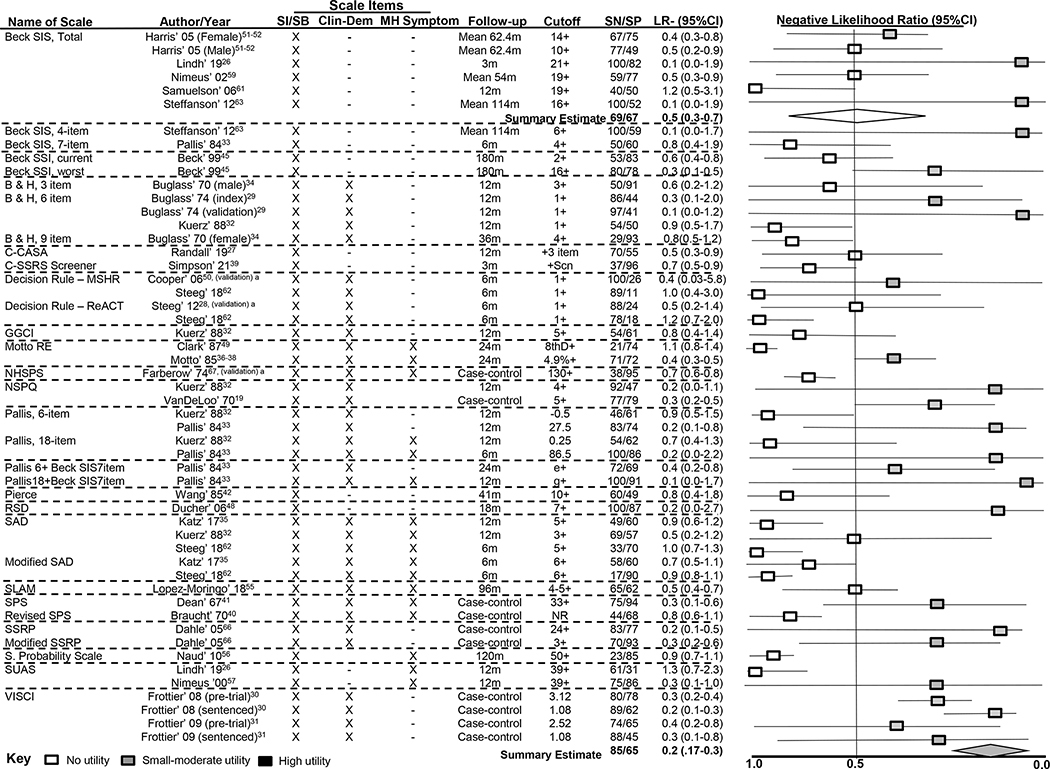
Data Extraction: Three reviewers in duplicate assessed full texts to determine eligibility and extracted data from included studies. Positive (LR+) and negative likelihood ratio (LR-) and 95% CIs were calculated for each instrument.
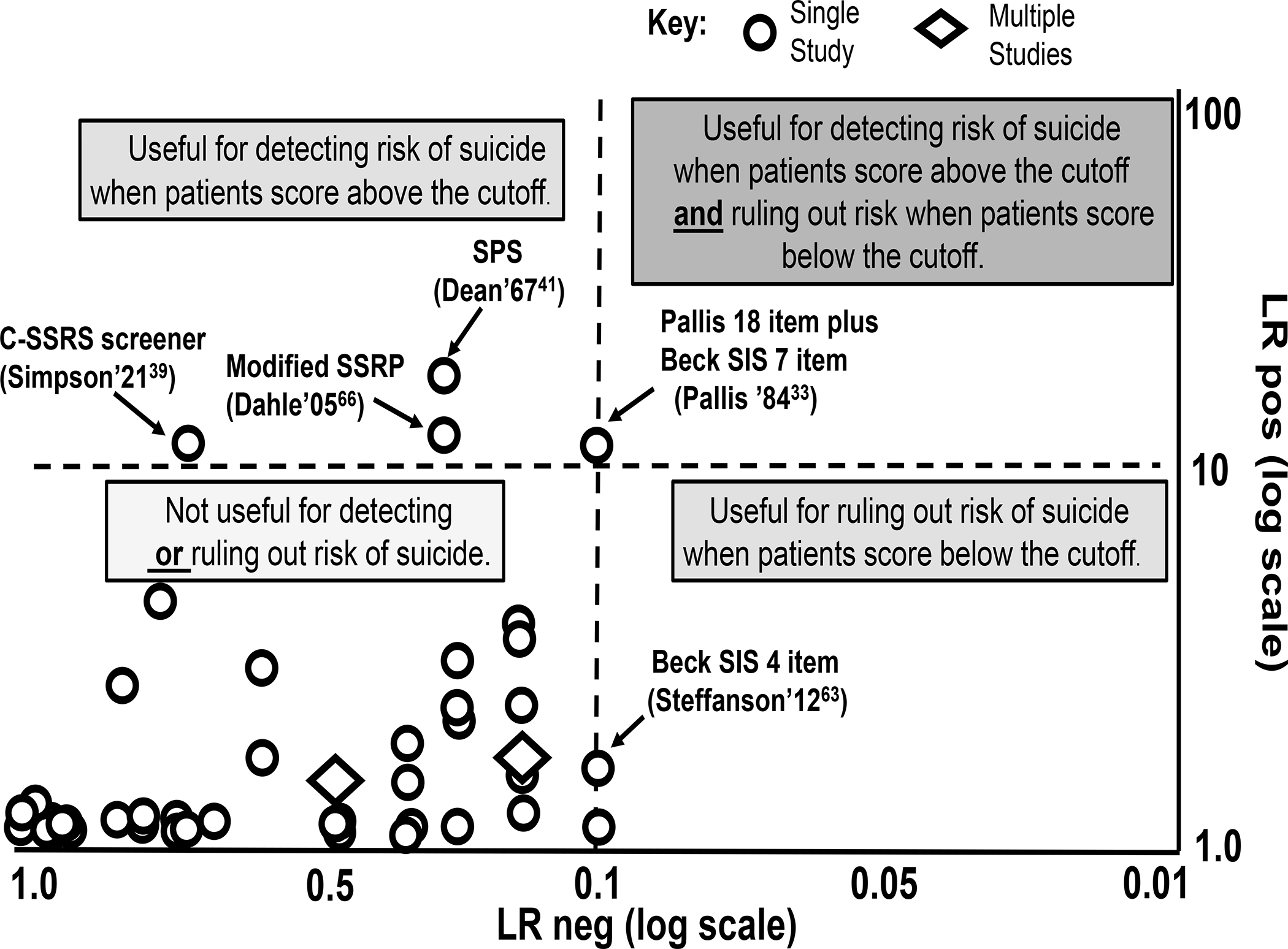
Results: Thirty studies met inclusion criteria. Most instruments showed minimal utility to detect or rule out risk of suicide, with LR+ ≤ 2.0 and LR- ≥ 0.5. A few instruments had a high utility for improving risk detection in emergency department, inpatient mental health, and prison settings when patients scored above the cutoff (LR+ > 10). For example, among patients discharged from an emergency department, the Columbia Suicide Severity Rating Scale-Clinical Practice Screener had a LR+ of 10.3 (95% CI, 6.3-16.8) at 3-month follow-up. The clinical utility of the instruments depends on the pretest probability of suicide in the setting. Because studies spanned over 6 decades, the findings are at risk for secular trends.
Discussion: We identified several instruments that may hold promise for detecting risk of suicide in emergency department, inpatient mental health, or prison settings. The utility of the instrument hinges, in part, on baseline suicide risk.
Registration: PROSPERO: CRD42021285528.
© Copyright 2022 Physicians Postgraduate Press, Inc.
Conflict of interest statement
Figures
Similar articles
-
Neuroimaging for the evaluation of chronic headaches: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(26):1-57. Epub 2010 Dec 1. Ont Health Technol Assess Ser. 2010. PMID: 23074404 Free PMC article.
-
Recovery schools for improving behavioral and academic outcomes among students in recovery from substance use disorders: a systematic review.Campbell Syst Rev. 2018 Oct 4;14(1):1-86. doi: 10.4073/csr.2018.9. eCollection 2018. Campbell Syst Rev. 2018. PMID: 37131375 Free PMC article.
-
Depression and Suicide Risk Screening: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force.JAMA. 2023 Jun 20;329(23):2068-2085. doi: 10.1001/jama.2023.7787. JAMA. 2023. PMID: 37338873
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups.Dan Med Bull. 2007 Nov;54(4):306-69. Dan Med Bull. 2007. PMID: 18208680 Review.
Cited by
-
Practitioners' perspective: a mixed-methods study on dealing with suicidality from the perspective of oncological healthcare professionals.J Cancer Res Clin Oncol. 2025 Jan 28;151(2):54. doi: 10.1007/s00432-025-06106-z. J Cancer Res Clin Oncol. 2025. PMID: 39875636 Free PMC article.
-
Health Service Protection vis-à-vis the Detection of Psychosocial Risks of Suicide during the Years 2019-2021.Healthcare (Basel). 2023 May 22;11(10):1505. doi: 10.3390/healthcare11101505. Healthcare (Basel). 2023. PMID: 37239791 Free PMC article.
-
Comparison of two suicide screening instruments for identifying high-risk individuals in prison.Front Psychiatry. 2024 Jun 27;15:1362928. doi: 10.3389/fpsyt.2024.1362928. eCollection 2024. Front Psychiatry. 2024. PMID: 38993384 Free PMC article.
-
Investigating the Differential Impact of Psychosocial Factors by Patient Characteristics and Demographics on Veteran Suicide Risk Through Machine Learning Extraction of Cross-Modal Interactions.Pac Symp Biocomput. 2025;30:167-184. doi: 10.1142/9789819807024_0013. Pac Symp Biocomput. 2025. PMID: 39670369 Free PMC article.
-
Clinician Suicide Risk Assessment for Prediction of Suicide Attempt in a Large Health Care System.JAMA Psychiatry. 2025 Jun 1;82(6):599-608. doi: 10.1001/jamapsychiatry.2025.0325. JAMA Psychiatry. 2025. PMID: 40202745
References
-
- Brown G A review of suicide assessment measures for intervention research with adults and older adults. https://www.sprc.org/resources-programs/review-suicide-assessment-measur... Accessed December 9, 2021.
-
- The Joint Commission. National Patient Safety Goal for suicide prevention. R3 Report. https://www.jointcommission.org/-/media/tjc/documents/standards/r3-repor... Accessed December 9, 2021
-
- Saab MM, Murphy M, Meehan E, et al. Suicide and self-harm risk assessment: A systematic review of prospective research. Arch Suicide Res. 2021:1–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
