

Toward personalized immunotherapy in sepsis: The PROVIDE randomized clinical trial
- PMID: 36384100
- PMCID: PMC9729870
- DOI: 10.1016/j.xcrm.2022.100817
Toward personalized immunotherapy in sepsis: The PROVIDE randomized clinical trial
Abstract
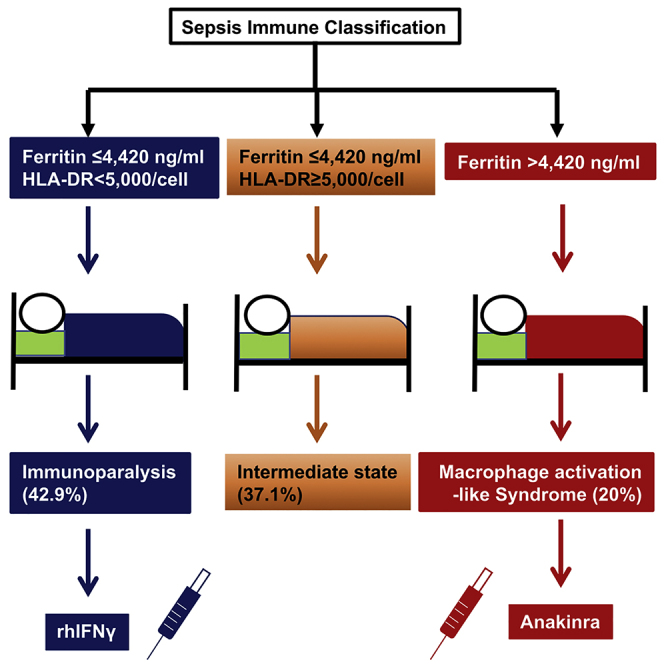
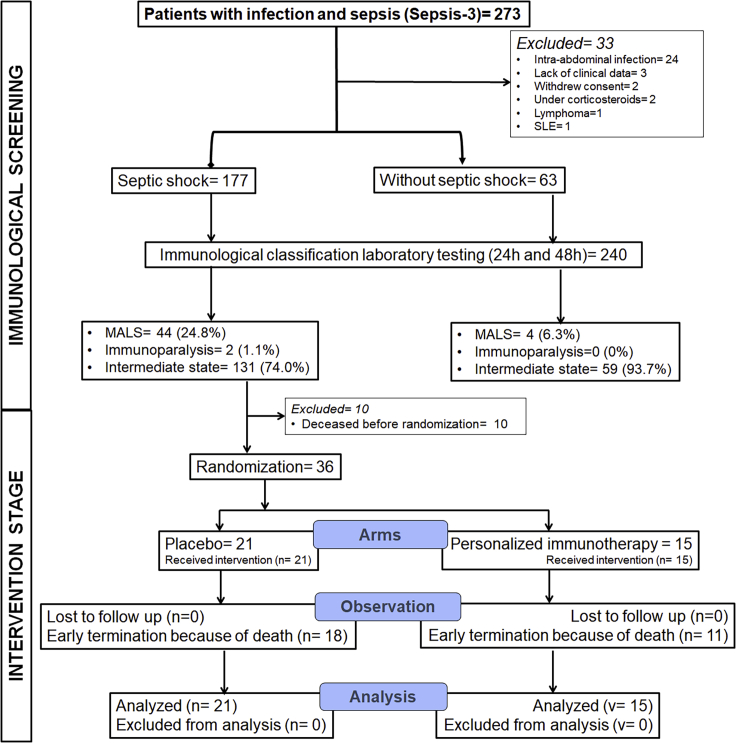
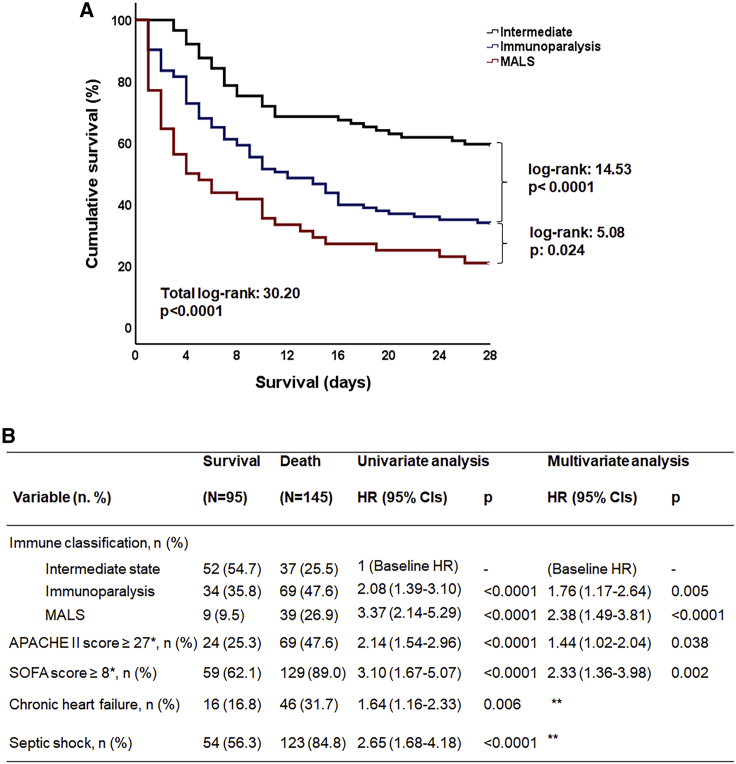
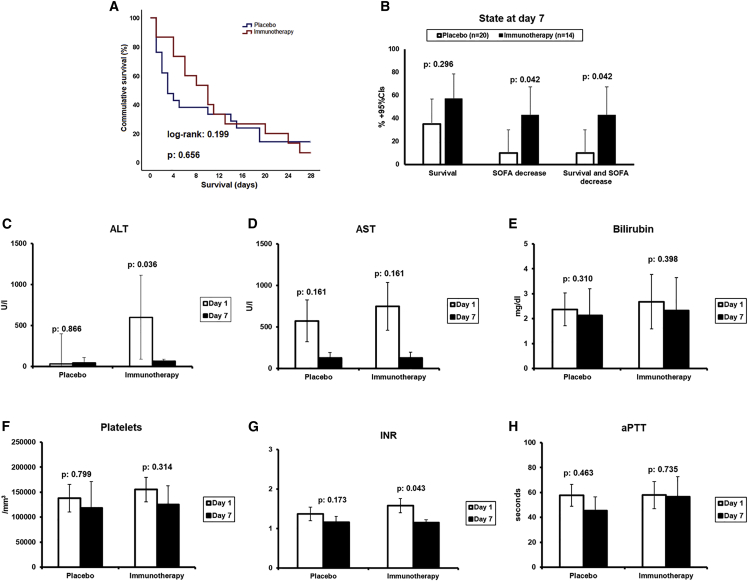
The state of immune activation may guide targeted immunotherapy in sepsis. In a double-blind, double-dummy randomized clinical study, 240 patients with sepsis due to lung infection, bacteremia, or acute cholangitis were subjected to measurements of serum ferritin and HLA-DR/CD14. Patients with macrophage activation-like syndrome (MALS) or immunoparalysis were randomized to treatment with anakinra or recombinant interferon-gamma or placebo. Twenty-eight-day mortality was the primary endpoint; sepsis immune classification was the secondary endpoint. Using ferritin >4,420 ng/mL and <5,000 HLA-DR receptors/monocytes as biomarkers, patients were classified into MALS (20.0%), immunoparalysis (42.9%), and intermediate (37.1%). Mortality was 79.1%, 66.9%, and 41.6%, respectively. Survival after 7 days with SOFA score decrease was achieved in 42.9% of patients of the immunotherapy arm and 10.0% of the placebo arm (p = 0.042). Three independent immune classification strata are recognized in sepsis. MALS and immunoparalysis are proposed as stratification for personalized adjuvant immunotherapy. Clinicaltrials.gov registration NCT03332225.
Keywords: ferritin; immunoparalysis; macrophage activation; monocytes; mortality; sepsis.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests G.D. has acted as Advisor/Lecturer for Abbvie, Bristol-Myers Squibb, Gilead, Novartis, Roche, Amgen, MSD, Janssen, Ipsen, Genkyotex, Sobi, and Pfizer; has received grant support from Bristol-Myers Squib, Gilead, Roche, Janssen, Abbvie, and Bayer; and was or is currently principal investigator in national and international protocols sponsored by Abbvie, Bristol-Myers Squibb, Novartis, Gilead, Novo Nordisk, Genkyotex, Regulus Therapeutics Inc, Tiziana Life Sciences, Bayer, Astellas, Ipsen, Pfizer, Amyndas Pharamaceuticals, CymaBay Therapeutics Inc., and Roche. M.G.N. is supported by an ERC Advanced Grant (#833247) and a Spinoza grant of the Netherlands Organization for Scientific Research. He is a scientific founder of TTxD and has received independent educational grants from TTxD, GSK, Ono Pharma, and ViiV HealthCare. E.J.G.-B. has received honoraria from Abbott CH, bioMérieux, ThermoFisherBrahms GmbH, GSK, InflaRx GmbH, Sobi, and XBiotech Inc; independent educational grants from Abbott CH, AxisShield, bioMérieux Inc, InflaRx GmbH, Johnson & Johnson, MSD, Sobi, and XBiotech Inc.; and funding from the Horizon2020 Marie-Curie Project European Sepsis Academy (granted to the National and Kapodistrian University of Athens), the Horizon 2020 European Grants ImmunoSep and RISCinCOVID (granted to the Hellenic Institute for the Study of Sepsis), and the Horizon Health European Grant EPIC-CROWN-2 (granted to the Hellenic Institute for the Study of Sepsis).
Figures

Comment in
-
Identifying inflammatory phenotypes to target mechanism-specific treatments in sepsis.Cell Rep Med. 2022 Nov 15;3(11):100823. doi: 10.1016/j.xcrm.2022.100823. Cell Rep Med. 2022. PMID: 36384087 Free PMC article.
References
-
- Rhodes A., Evans L.E., Alhazzani W., Levy M.M., Antonelli M., Ferrer R., Kumar A., Sevransky J.E., Sprung C.L., Nunnally M.E., et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017;45:486–552. - PubMed
-
- Minoia F., Davì S., Horne A., Demirkaya E., Bovis F., Li C., Lehmberg K., Weitzman S., Insalaco A., Wouters C., et al. Clinical features, treatment, and outcome of macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: a multinational, multicenter study of 362 patients. Arthritis Rheumatol. 2014;66:3160–3169. - PubMed
-
- Fardet L., Galicier L., Lambotte O., Marzac C., Aumont C., Chahwan D., Coppo P., Hejblum G. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014;66:2613–2620. - PubMed
-
- Shakoory B., Carcillo J.A., Chatham W.W., Amdur R.L., Zhao H., Dinarello C.A., Cron R.Q., Opal S.M. Interleukin-1 receptor blockade is associated with reduced mortality in sepsis patients with features of macrophage activation syndrome: reanalysis of a prior phase III trial. Crit. Care Med. 2016;44:275–281. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
