

Prevention and management of secondary central nervous system lymphoma
- PMID: 36384246
- PMCID: PMC9973486
- DOI: 10.3324/haematol.2022.281457
Prevention and management of secondary central nervous system lymphoma
Abstract
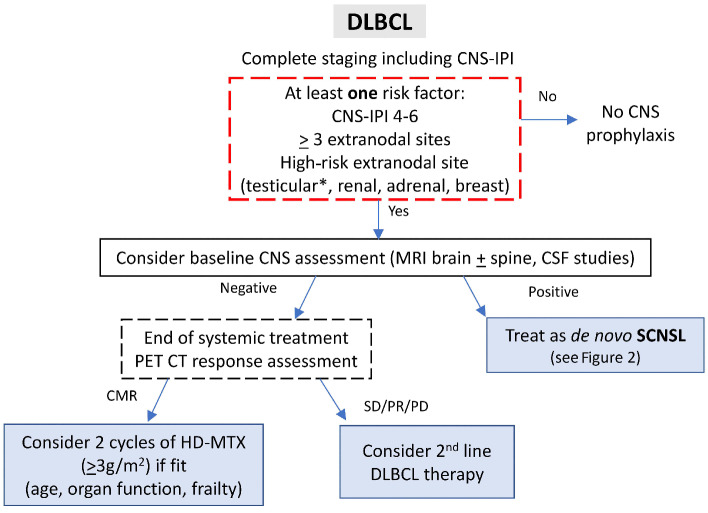
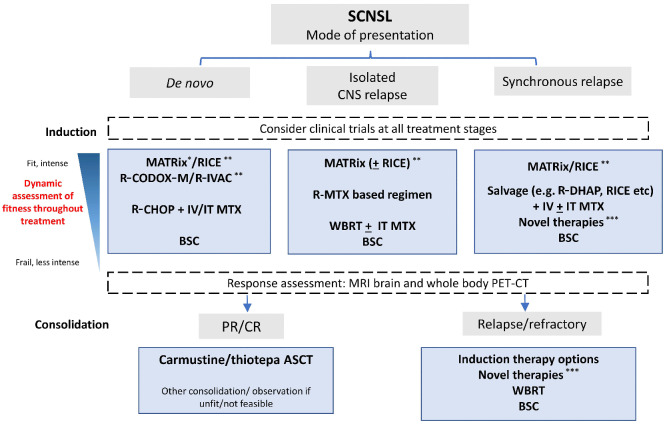
Secondary central nervous system (CNS) lymphoma (SCNSL) is defined by the involvement of the CNS, either at the time of initial diagnosis of systemic lymphoma or in the setting of relapse, and can be either isolated or with synchronous systemic disease. The risk of CNS involvement in patients with diffuse large B-cell lymphoma is approximately 5%; however, certain clinical and biological features have been associated with a risk of up to 15%. There has been growing interest in improving the definition of patients at increased risk of CNS relapse, as well as identifying effective prophylactic strategies to prevent it. SCNSL often occurs within months of the initial diagnosis of lymphoma, suggesting the presence of occult disease at diagnosis in many cases. The differing presentations of SCNSL create the therapeutic challenge of controlling both the systemic disease and the CNS disease, which uniquely requires agents that penetrate the blood-brain barrier. Outcomes are generally poor with a median overall survival of approximately 6 months in retrospective series, particularly in those patients presenting with SCNSL after prior therapy. Prospective studies of intensive chemotherapy regimens containing high-dose methotrexate, followed by hematopoietic stem cell transplantation have shown the most favorable outcomes, especially for patients receiving thiotepa-based conditioning regimens. However, a proportion of patients will not respond to induction therapies or will subsequently relapse, indicating the need for more effective treatment strategies. In this review we focus on the identification of high-risk patients, prophylactic strategies and recent treatment approaches for SCNSL. The incorporation of novel agents in immunochemotherapy deserves further study in prospective trials.
Figures
References
-
- Hollender A, Kvaloy S, Lote K, Nome O, Holte H. Prognostic factors in 140 adult patients with non-Hodgkin's lymphoma with systemic central nervous system (CNS) involvement. A single centre analysis. Eur J Cancer. 2000;36(14):1762-1768. - PubMed
-
- Schmitz N, Zeynalova S, Nickelsen M, et al. . CNS International Prognostic Index: a risk model for CNS relapse in patients with diffuse large B-cell lymphoma treated with R-CHOP. J Clin Oncol. 2016;34(26):3150-3156. - PubMed
-
- Ferreri AJ, Donadoni G, Cabras MG, et al. . High doses of antimetabolites followed by high-dose sequential chemoimmunotherapy and autologous stem-cell transplantation in patients with systemic B-cell lymphoma and secondary CNS involvement: final results of a multicenter phase II trial. J Clin Oncol. 2015;33(33):3903-3010. - PubMed
-
- Wilson MR, Eyre TA, Kirkwood AA, et al. . Timing of high-dose methotrexate CNS prophylaxis in DLBCL: a multicenter international analysis of 1384 patients. Blood. 2022;139(16):2499-2511. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
