

Anti-NMDA receptor encephalitis and MOG-associated demyelination - a case report with long-term follow-up and a systematic review
- PMID: 36384491
- PMCID: PMC9667590
- DOI: 10.1186/s12883-022-02974-x
Anti-NMDA receptor encephalitis and MOG-associated demyelination - a case report with long-term follow-up and a systematic review
Abstract
Background: Overlap syndromes of anti-NMDA receptor encephalitis and MOG-mediated demyelination have been reported. In this case we provide a long-term longitudinal follow-up of clinical and imaging characteristics as well as of antibody dynamics.
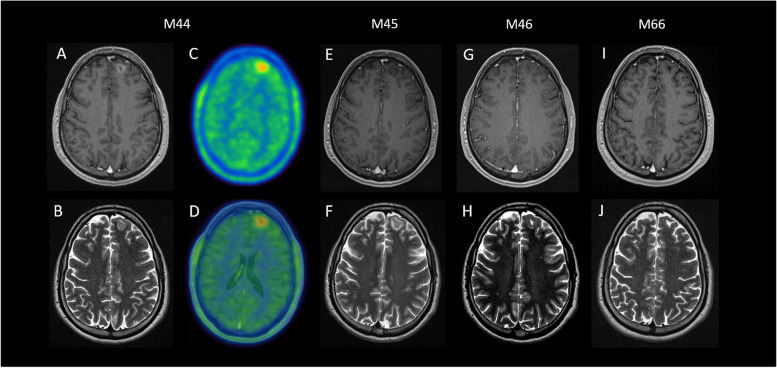
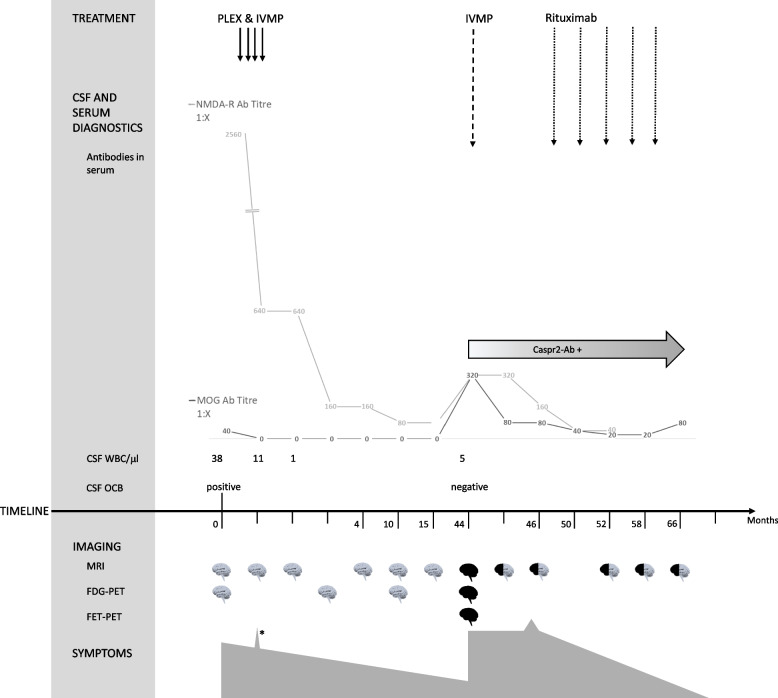
Case presentation: We report a 32-year-old male patient who presented with psychosis, decreased consciousness and movement disorders and was tested positive for anti-NMDA receptor antibodies. Forty-four months after symptom onset and diagnosis of autoimmune encephalitis, he suffered from relapse. At this time, the patient developed anti-MOG and anti-Caspr2 antibodies. Treatment with plasmapheresis, steroids and rituximab eventually led to substantial clinical and radiological improvement. Anti-Caspr2 antibodies persisted, anti-NMDA receptor antibodies decreased, while anti-MOG antibodies turned negative again.
Conclusion: We provide long-term longitudinal follow-up of a patient with anti-NMDA receptor encephalitis who developed triple antibody positivity at the time of relapse. Antibody dynamics were associated with clinical disease course.
Keywords: Anti-N-Methyl-D-Aspartate; Case report; Demyelination; Encephalitis; Myelin Oligodendrocyte Glycoprotein; NMDA.
© 2022. The Author(s).
Conflict of interest statement
Klaus Berek has participated in meetings sponsored by, received travel funding from or received honoraria for acting as an advisor/speaker for Roche, Biogen, TEVA and Sanofi.
Astrid Grams reports no conflicts of interest.
Christian Uprimny reports no conflicts of interest.
Manuela Prieschl reports no conflicts of interest.
Melanie Ramberger reports no conflicts of interest.
Iris Unterberger reports no conflicts of interest.
Florian Deisenhammer has participated in meetings sponsored by or received honoraria for acting as an advisor/speaker for Almirall, Alexion, Biogen, Celgene, Genzyme-Sanofi, Merck, Novartis Pharma, Roche, and TEVA ratiopharm. His institution has received research grants from Biogen and Genzyme Sanofi. He is section editor of the MSARD Journal (Multiple Sclerosis and Related Disorders) and review editor of Frontiers Neurology.
Markus Reindl is supported by research grants from the Austrian Science Fund (FWF project P32699), the Austrian Research Promotion Agency, Euroimmun and Roche; consulting fees and advisory board from Roche (to institution). He works at the Clinical Department of Medical University of Innsbruck which offers diagnostic testing for MOG and other autoantibodies.
Harald Hegen has participated in meetings sponsored by, received speaker honoraria or travel funding from Biogen, Celgene, Merck, Novartis, Sanofi-Genzyme, Siemens, Teva, and received honoraria for acting as consultant for Biogen, Celgene, Novartis and Teva.
Figures
References
-
- Dalmau J, Armangue T, Planaguma J, Radosevic M, Mannara F, Leypoldt F, et al. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. Lancet Neurol. 2019;18(11):1045–1057. - PubMed
-
- Aoe S, Kokudo Y, Takata T, Kobara H, Yamamoto M, Touge T, et al. Repeated anti-N-methyl-D-aspartate receptor encephalitis coexisting with anti-myelin oligodendrocyte glycoprotein antibody-associated diseases: a case report. Mult Scler Relat Disord. 2019;35:182–184. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
