

Diabetes mellitus in transfemoral transcatheter aortic valve implantation: a propensity matched analysis
- PMID: 36384656
- PMCID: PMC9670618
- DOI: 10.1186/s12933-022-01654-x
Diabetes mellitus in transfemoral transcatheter aortic valve implantation: a propensity matched analysis
Abstract
Background: Diabetes Mellitus (DM) affects a third of patients with symptomatic severe aortic valve stenosis undergoing transcatheter aortic valve implantation (TAVI). DM is a well-known risk factor for cardiac surgery, but its prognostic impact in TAVI patients remains controversial. This study aimed to evaluate outcomes in diabetic patients undergoing TAVI.
Methods: This multicentre registry includes data of > 12,000 patients undergoing transfemoral TAVI. We assessed baseline patient characteristics and clinical outcomes in patients with DM and without DM. Clinical outcomes were defined by the second valve academic research consortium. Propensity score matching was applied to minimize potential confounding.
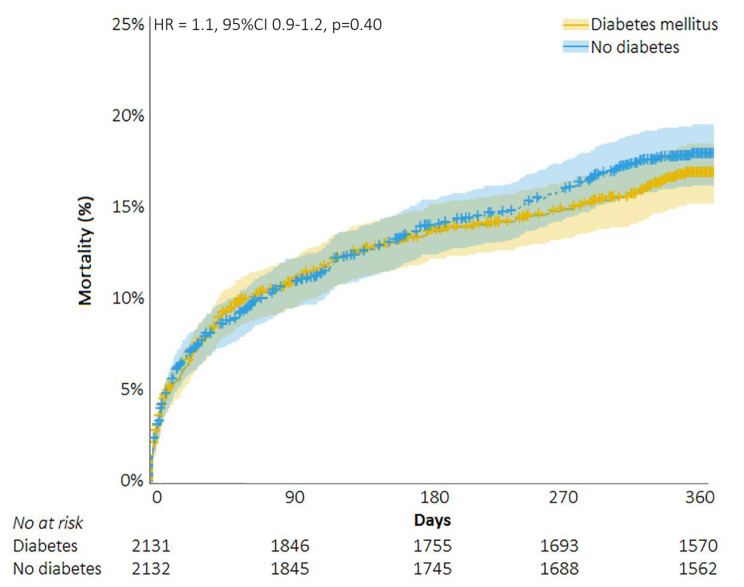
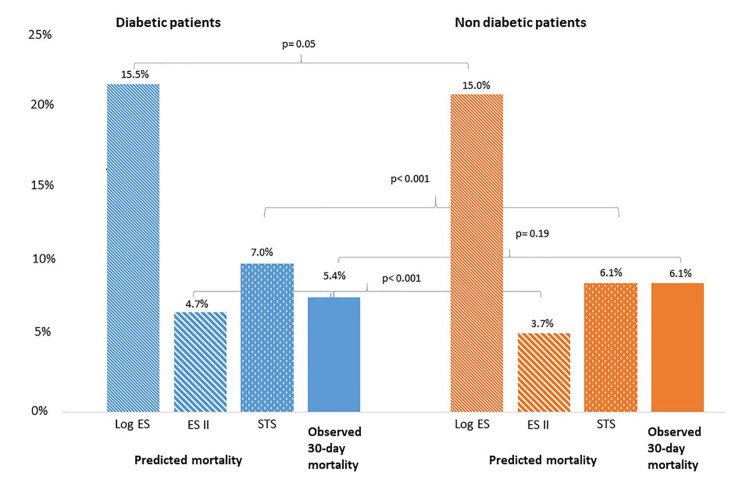
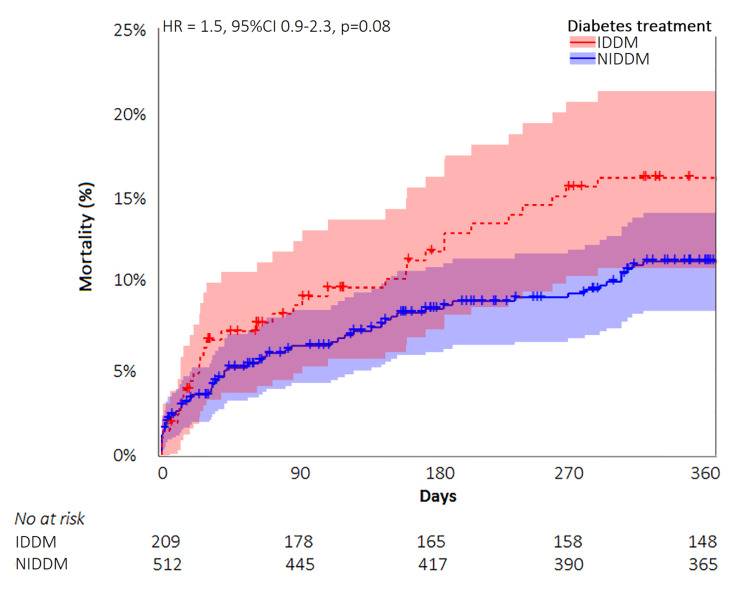
Results: Of the 11,440 patients included, 31% (n = 3550) had DM and 69% (n = 7890) did not have DM. Diabetic patients were younger but had an overall worse cardiovascular risk profile than non-diabetic patients. All-cause mortality rates were comparable at 30 days (4.5% vs. 4.9%, RR 0.9, 95%CI 0.8-1.1, p = 0.43) and at one year (17.5% vs. 17.4%, RR 1.0, 95%CI 0.9-1.1, p = 0.86) in the unmatched population. Propensity score matching obtained 3281 patient-pairs. Also in the matched population, mortality rates were comparable at 30 days (4.7% vs. 4.3%, RR 1.1, 95%CI 0.9-1.4, p = 0.38) and one year (17.3% vs. 16.2%, RR 1.1, 95%CI 0.9-1.2, p = 0.37). Other clinical outcomes including stroke, major bleeding, myocardial infarction and permanent pacemaker implantation, were comparable between patients with DM and without DM. Insulin treated diabetics (n = 314) showed a trend to higher mortality compared with non-insulin treated diabetics (n = 701, Hazard Ratio 1.5, 95%CI 0.9-2.3, p = 0.08). EuroSCORE II was the most accurate risk score and underestimated 30-day mortality with an observed-expected ratio of 1.15 in DM patients, STS-PROM overestimated actual mortality with a ratio of 0.77 and Logistic EuroSCORE with 0.35.
Conclusion: DM was not associated with mortality during the first year after TAVI. DM patients undergoing TAVI had low rates of mortality and other adverse clinical outcomes, comparable to non-DM TAVI patients. Our results underscore the safety of TAVI treatment in DM patients.
Trial registration: The study is registered at clinicaltrials.gov (NCT03588247).
Keywords: Aortic valve stenosis; Bleeding; Diabetes mellitus; Insulin; Mortality; Stroke; TAVI; Transcatheter aortic valve replacement.
© 2022. The Author(s).
Conflict of interest statement
Dr. de Brito Jr is a proctor for Edwards Lifesciences and Medtronic. Dr. Amat-Santos is a proctor for Boston Scientific. Dr. Barbanti is consultant for Edwards Lifesciences, and received speaker honoraria from Medtronic and Biotronik. Dr. Latib is a consultant for Medtronic, and has received honoraria from Abbott Vascular. Dr. Baan receives an unrestricted research grant from Edwards Lifesciences. The remaining authors have no relevant disclosures.
Figures
References
-
- Parakh K. Diabetes and mortality risk after acute coronary syndromes. J. Am. Med. Assoc. 2007. p. 2367–8. - PubMed
-
- Sarwar N, Gao P, Kondapally Seshasai SR, Gobin R, Kaptoge S, Di Angelantonio E, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375:2215–22. doi: 10.1016/S0140-6736(10)60484-9. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
