

Burden of respiratory syncytial virus infection in older and high-risk adults: a systematic review and meta-analysis of the evidence from developed countries
- PMID: 36384703
- PMCID: PMC9724807
- DOI: 10.1183/16000617.0105-2022
Burden of respiratory syncytial virus infection in older and high-risk adults: a systematic review and meta-analysis of the evidence from developed countries
Abstract
Background: Respiratory syncytial virus (RSV) significantly impacts the health of older and high-risk adults (those with comorbidities). We aimed to synthesise the evidence on RSV disease burden and RSV-related healthcare utilisation in both populations.
Methods: We searched Embase and MEDLINE for papers published between 2000 and 2019 reporting the burden and clinical presentation of symptomatic RSV infection and the associated healthcare utilisation in developed countries in adults aged ≥60 years or at high risk. We calculated pooled estimates using random-effects inverse variance-weighted meta-analysis.
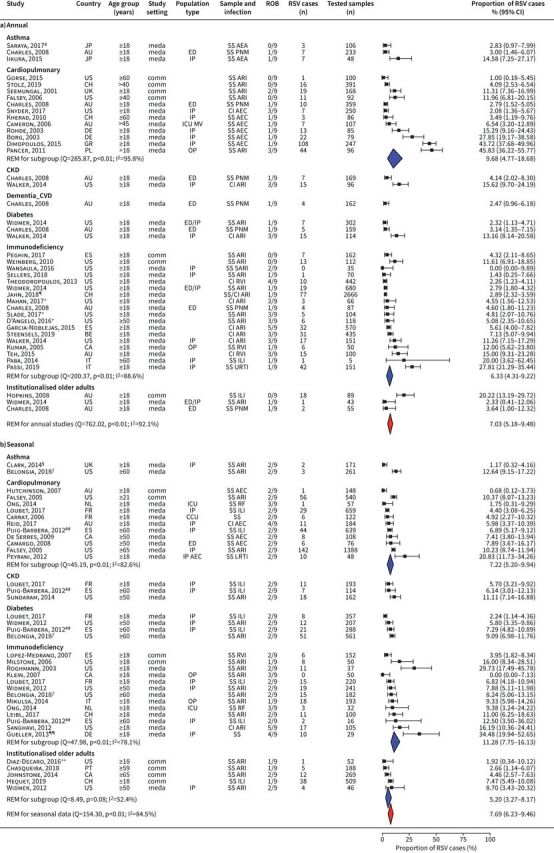
Results: 103 out of 3429 articles met the inclusion criteria. Among older adults, RSV caused 4.66% (95% CI 3.34-6.48%) of symptomatic respiratory infections in annual studies and 7.80% (95% CI 5.77-10.45%) in seasonal studies; RSV-related case fatality proportion (CFP) was 8.18% (95% CI 5.54-11.94%). Among high-risk adults, RSV caused 7.03% (95% CI 5.18-9.48%) of symptomatic respiratory infections in annual studies, and 7.69% (95% CI 6.23-9.46%) in seasonal studies; CFP was 9.88% (95% CI 6.66-14.43%). Data paucity impaired the calculation of estimates on population incidence, clinical presentation, severe outcomes and healthcare-related utilisation.
Conclusions: Older and high-risk adults frequently experience symptomatic RSV infection, with appreciable mortality; however, detailed data are lacking. Increased surveillance and research are needed to quantify population-based disease burden and facilitate RSV treatments and vaccine development.
Copyright ©The authors 2022.
Conflict of interest statement
Conflicts of interest: J.S. Nguyen-Van-Tam received no research funding, honoraria, or non-financial benefits, including travel for his role in this or related work. He was seconded less than full-time to the Department of Health and Social Care, England (DHSC) from October 2017 to March 2022, but performed this in his academic capacity at the University of Nottingham. The view expressed in this article are those of the authors and not necessarily those of DHSC. M. O'Leary and T.M.P Tran are employees of P95, a company that received consulting fees from Janssen, Pharmaceutical Companies of Johnson & Johnson. E.T. Martin received no research funding, honoraria, or non-financial benefits, including travel for his role in this or related work. E. Heijnen, B. Callendret and C. Comeaux are employees of Janssen Vaccines and Prevention BV. R. Fleischhackl is an employee of Janssen Research and Development. K. Weber is an employee of Janssen Global Medical Affairs, IDV.
Figures



References
-
- Troeger C, Blacker B, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 2018; 18: 1191–1210. doi: 10.1016/S1473-3099(18)30310-4 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous