

Non-contrast free-breathing 3D cardiovascular magnetic resonance angiography using REACT (relaxation-enhanced angiography without contrast) compared to contrast-enhanced steady-state magnetic resonance angiography in complex pediatric congenital heart disease at 3T
- PMID: 36384752
- PMCID: PMC9670549
- DOI: 10.1186/s12968-022-00895-9
Non-contrast free-breathing 3D cardiovascular magnetic resonance angiography using REACT (relaxation-enhanced angiography without contrast) compared to contrast-enhanced steady-state magnetic resonance angiography in complex pediatric congenital heart disease at 3T
Abstract
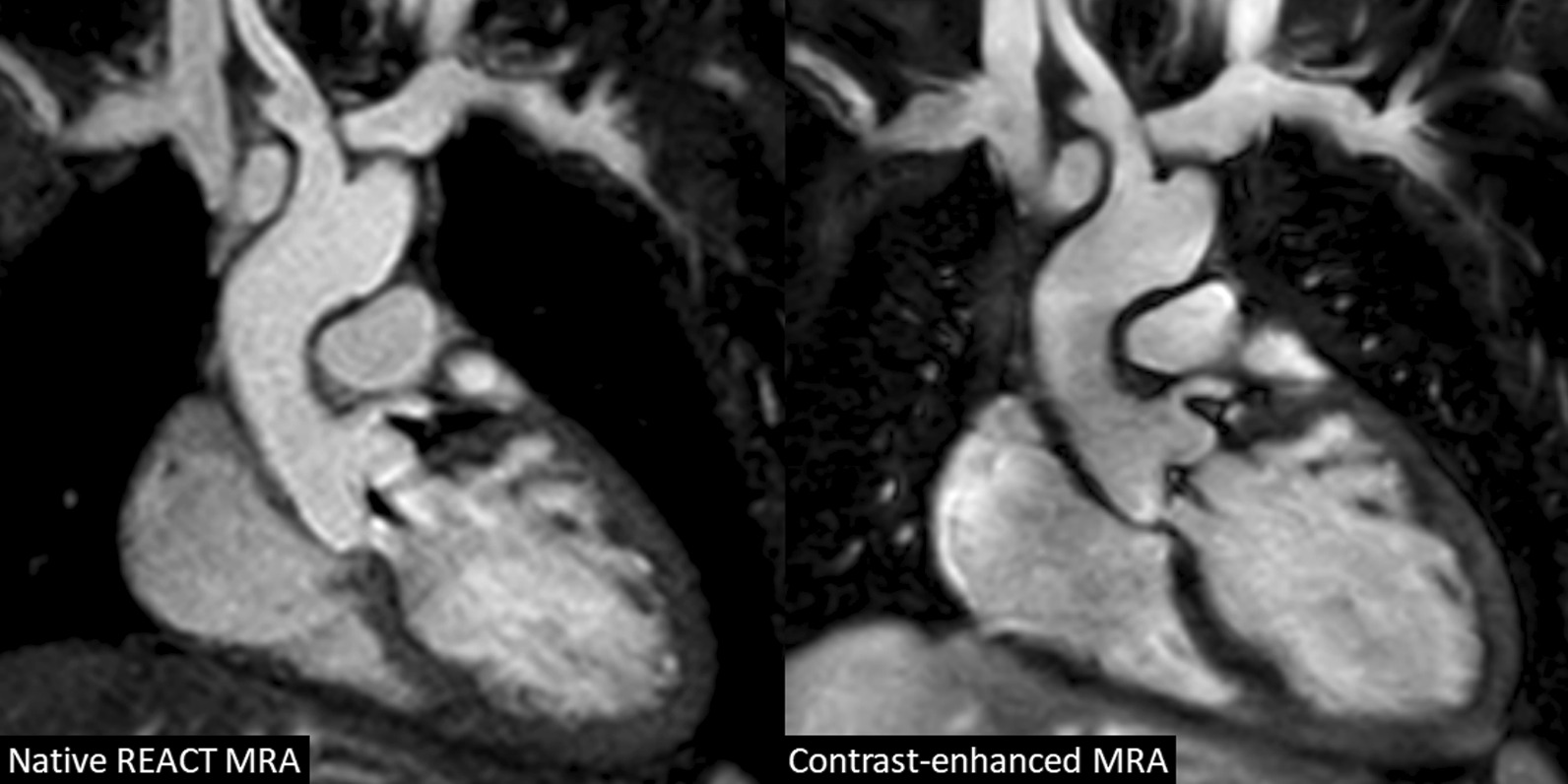
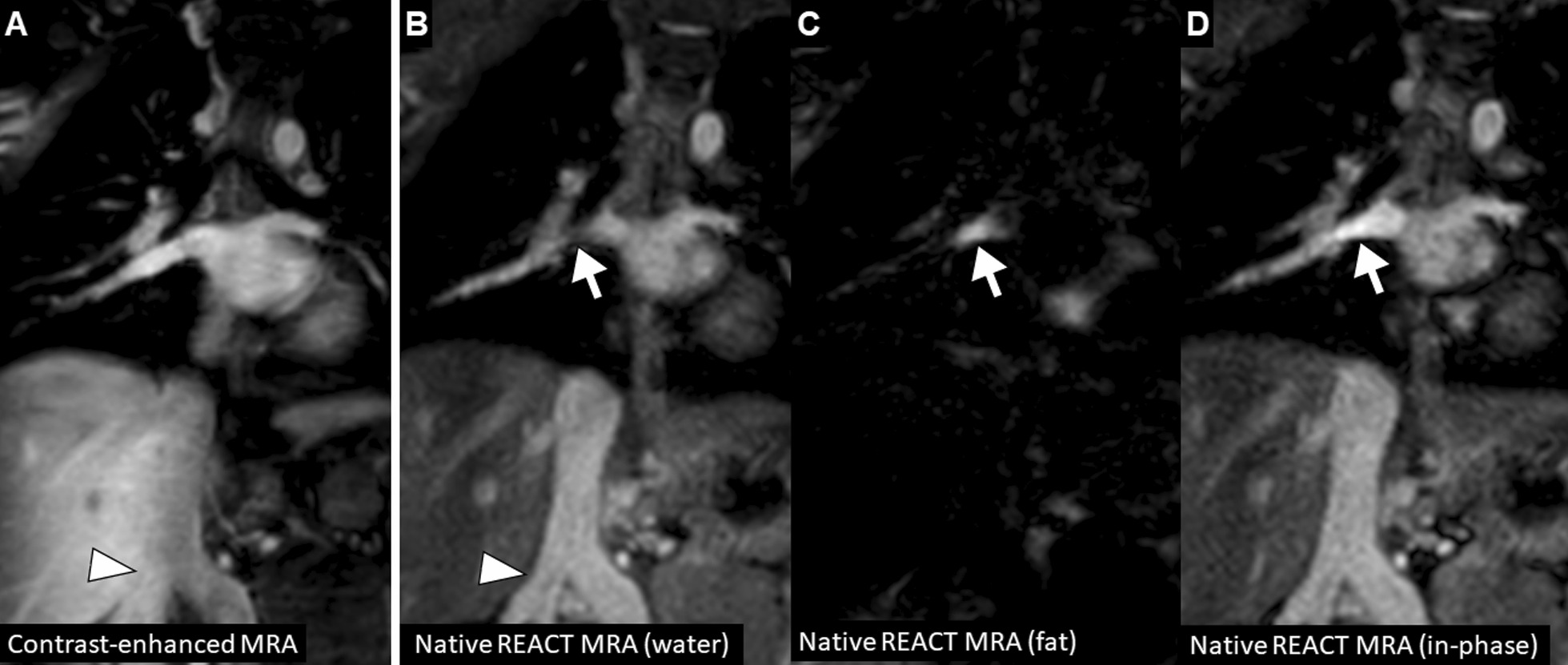
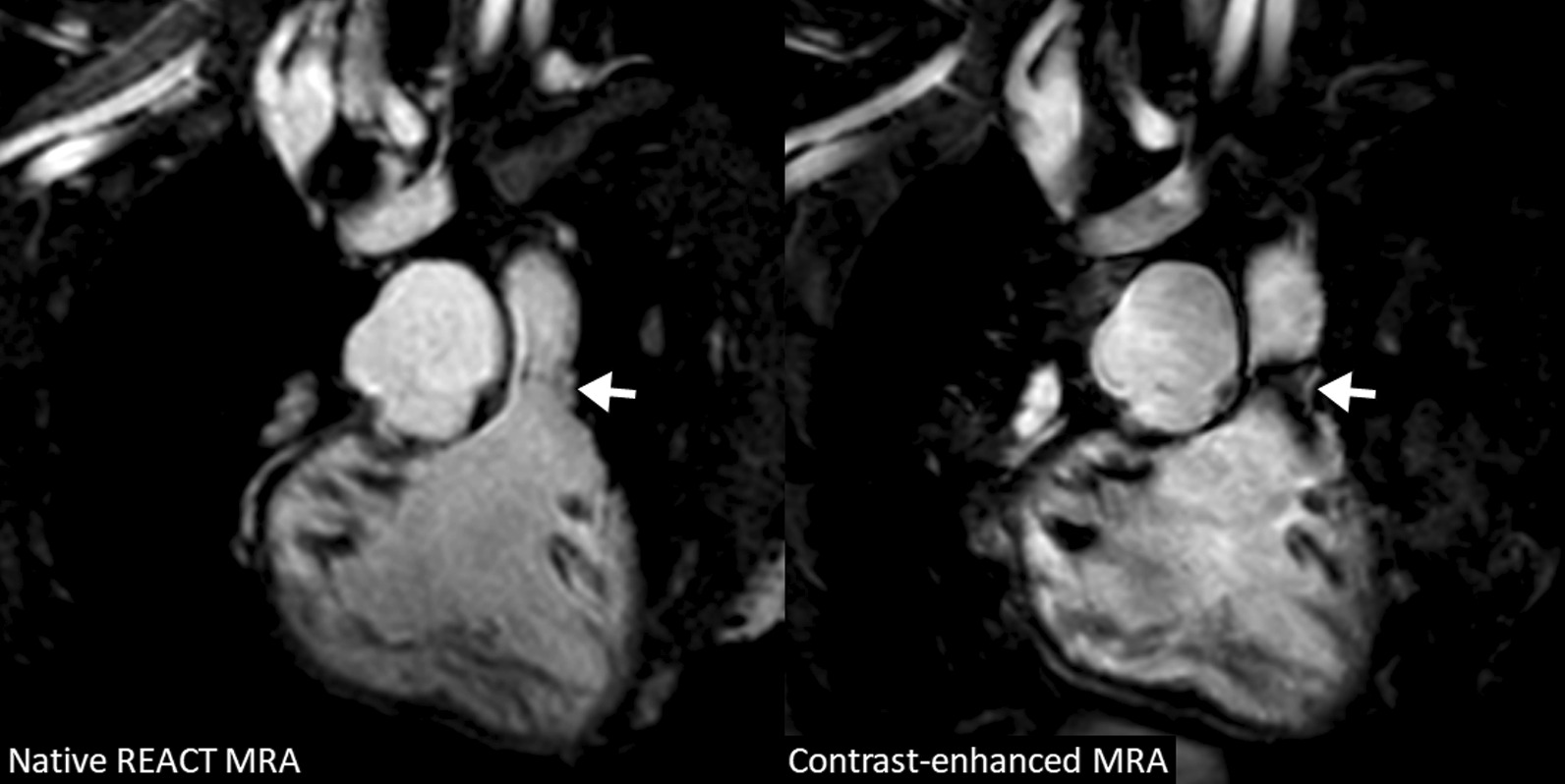
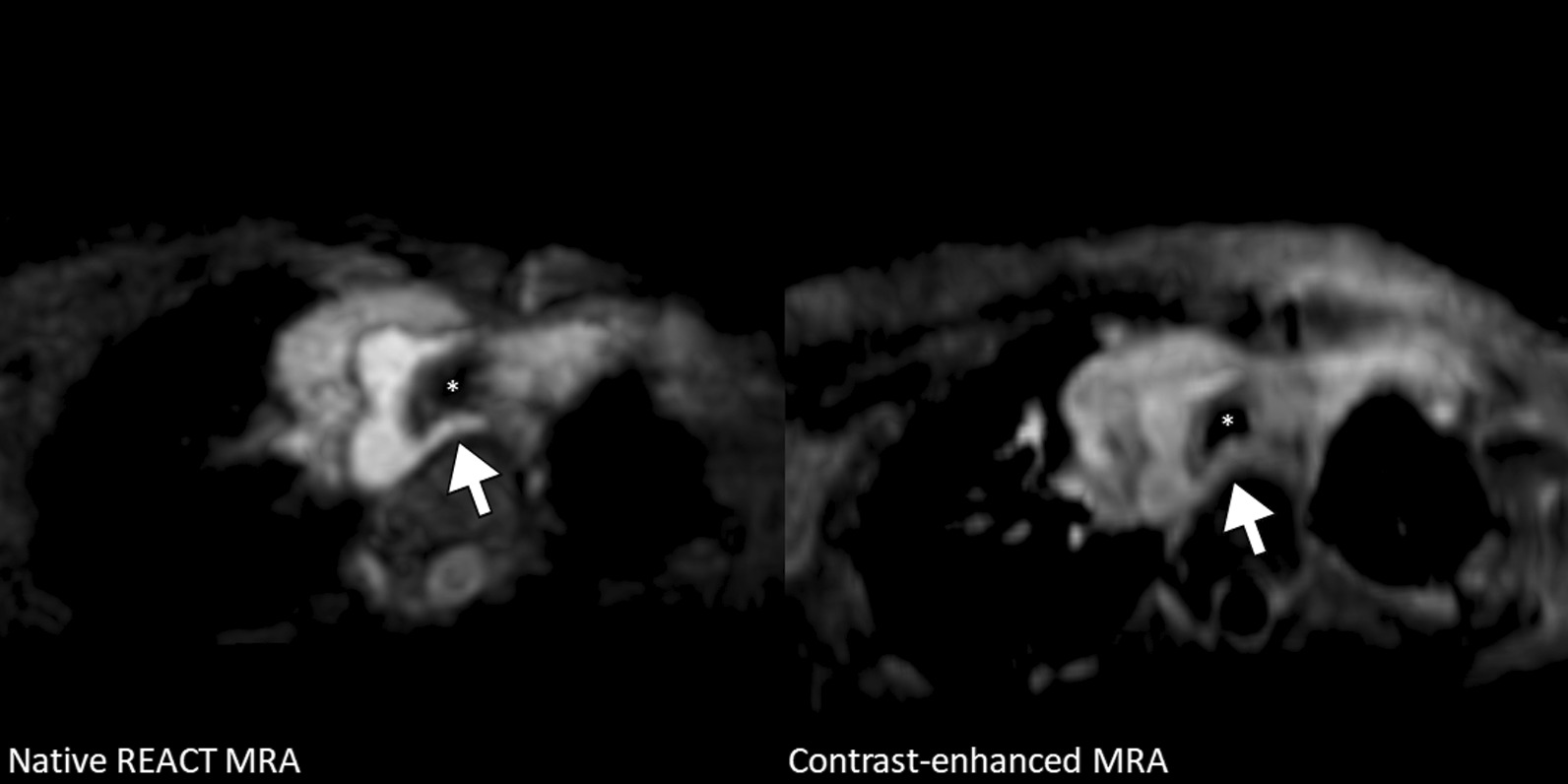
Background: To evaluate the great vessels in young children with complex congenital heart disease (CHD) using non-contrast cardiovascular magnetic resonance angiography (CMRA) based on three-dimensional relaxation-enhanced angiography without contrast (REACT) in comparison to contrast-enhanced steady-state CMRA.
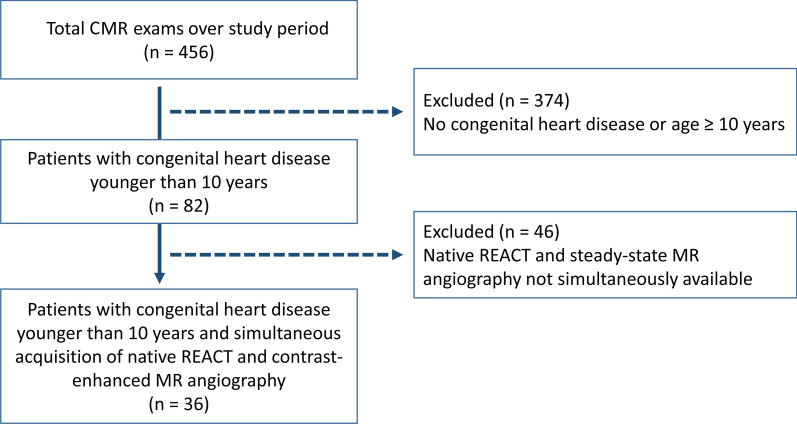
Methods: In this retrospective study from April to July 2021, respiratory- and electrocardiogram-gated native REACT CMRA was compared to contrast-enhanced single-phase steady-state CMRA in children with CHD who underwent CMRA at 3T under deep sedation. Vascular assessment included image quality (1 = non-diagnostic, 5 = excellent), vessel diameter, and diagnostic findings. For statistical analysis, paired t-test, Pearson correlation, Bland-Altman analysis, Wilcoxon test, and intraclass correlation coefficients (ICC) were applied.
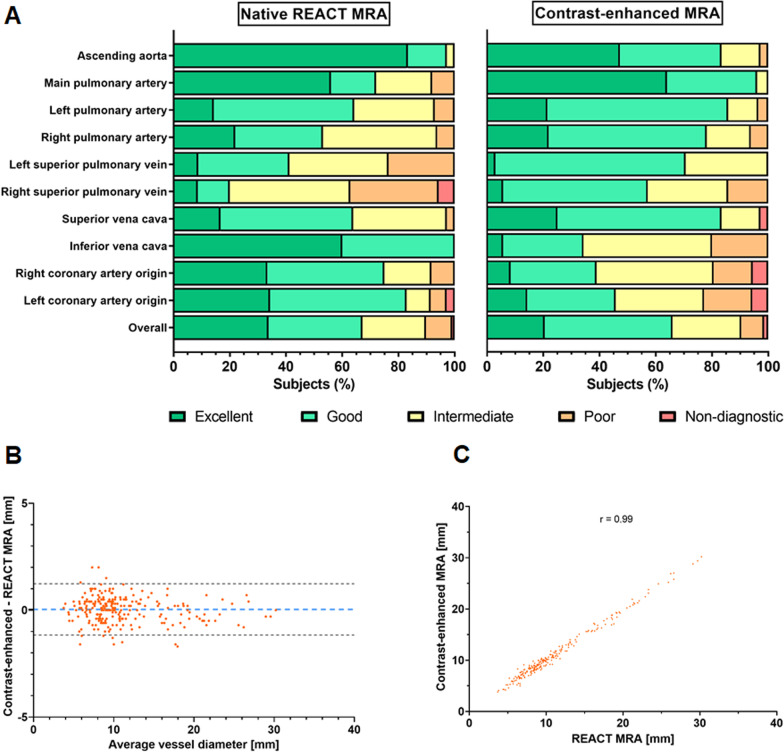
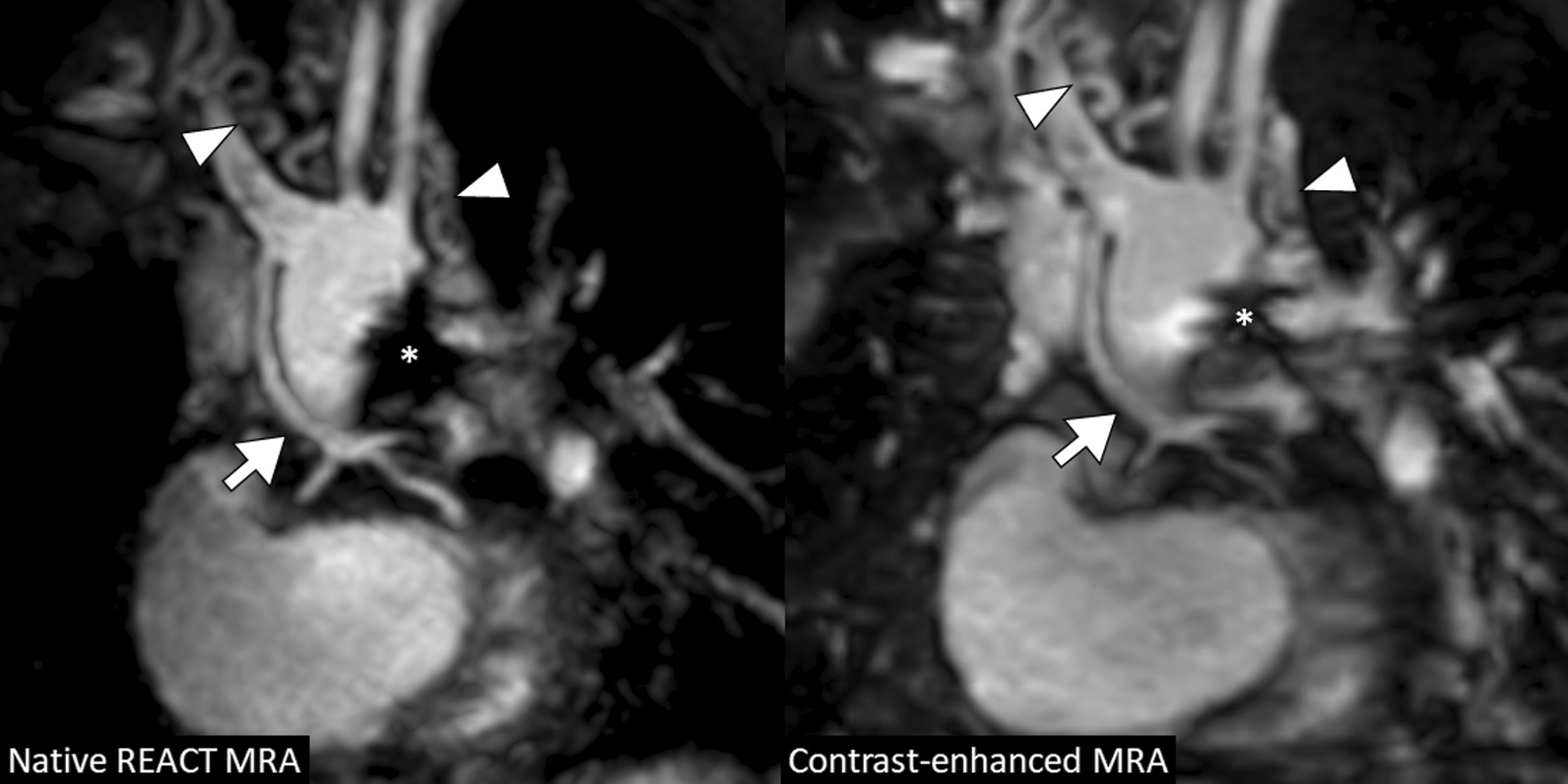
Results: Thirty-six young children with complex CHD (median 4 years, interquartile range, 2-5; 20 males) were included. Native REACT CMRA was obtained successfully in all patients (mean scan time: 4:22 ± 1:44 min). For all vessels assessed, diameters correlated strongly between both methods (Pearson r = 0.99; bias = 0.04 ± 0.61 mm) with high interobserver reproducibility (ICC: 0.99 for both CMRAs). Native REACT CMRA demonstrated comparable overall image quality to contrast-enhanced CMRA (3.9 ± 1.0 vs. 3.8 ± 0.9, P = 0.018). With REACT CMRA, better image quality was obtained at the ascending aorta (4.8 ± 0.5 vs. 4.3 ± 0.8, P < 0.001), coronary roots (e.g., left: 4.1 ± 1.0 vs. 3.3 ± 1.1, P = 0.001), and inferior vena cava (4.6 ± 0.5 vs. 3.2 ± 0.8, P < 0.001). In all patients, additional vascular findings were assessed equally with native REACT CMRA and the contrast-enhanced reference standard (n = 6).
Conclusion: In young children with complex CHD, REACT CMRA can provide gadolinium-free high image quality, accurate vascular measurements, and equivalent diagnostic quality compared to standard contrast-enhanced CMRA.
Keywords: Cardiovascular magnetic resonance angiography; Gadolinium-free; Non-contrast; Pediatric congenital heart disease; Relaxation-enhanced angiography without contrast.
© 2022. The Author(s).
Conflict of interest statement
S.Z., C.K., and O.W. (employees of Philips Healthcare) provided on-site technical support in setting up and adjusting the proposed native CMRA sequence. Nonemployee authors (A.I., J.A.L.) had full control of the data and information submitted for publication. There was no financial support from the industry for this study.
Figures


References
-
- Sachdeva R, Valente AM, Armstrong AK, Cook SC, Han BK, Lopez L, et al. ACC/AHA/ASE/HRS/ISACHD/SCAI/SCCT/SCMR/SOPE 2020 appropriate use criteria for multimodality imaging during the follow-up care of patients with congenital heart disease: a report of the American College of Cardiology Solution Set Oversight Committee and Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Pediatric Echocardiography. J Am Coll Cardiol. 2020;75:657–703. doi: 10.1016/j.jacc.2019.10.002. - DOI - PubMed
-
- Fratz S, Chung T, Greil GF, Samyn MM, Taylor AM, Valsangiacomo Buechel ER, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15:51. doi: 10.1186/1532-429X-15-51. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
