

Motor symptoms in genetic frontotemporal dementia: developing a new module for clinical rating scales
- PMID: 36385202
- PMCID: PMC9971048
- DOI: 10.1007/s00415-022-11442-y
Motor symptoms in genetic frontotemporal dementia: developing a new module for clinical rating scales
Abstract
Objective: To investigate the optimal method of adding motor features to a clinical rating scale for frontotemporal dementia (FTD).
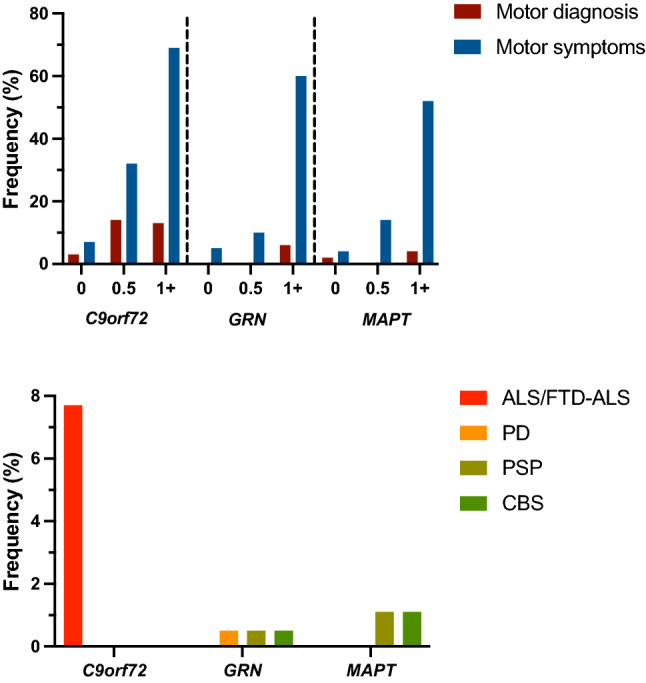
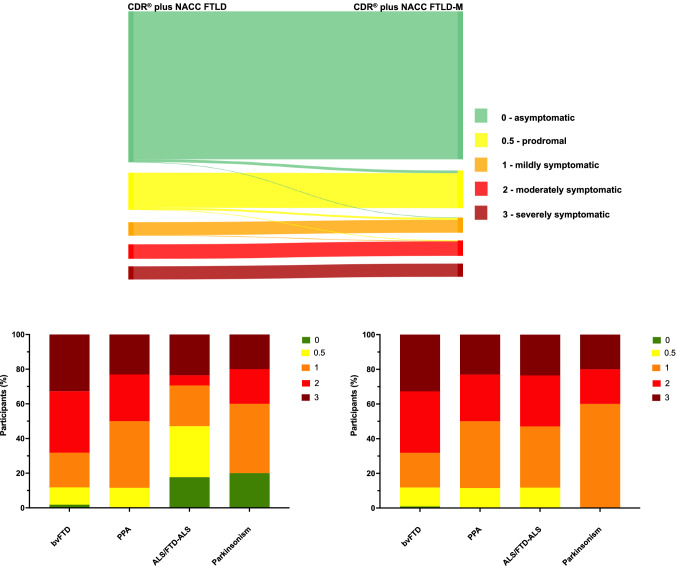
Methods: Eight hundred and thirty-two participants from the international multicentre Genetic FTD Initiative (GENFI) study were recruited: 522 mutation carriers (with C9orf72, GRN and MAPT mutations) and 310 mutation-negative controls. A standardised clinical questionnaire was used to assess eight motor symptoms (dysarthria, dysphagia, tremor, slowness, weakness, gait disorder, falls and functional difficulties using hands). Frequency and severity of each motor symptom was assessed, and a principal component analysis (PCA) was performed to identify how the different motor symptoms loaded together. Finally, addition of a motor component to the CDR® plus NACC FTLD was investigated (CDR® plus NACC FTLD-M).
Results: 24.3% of mutation carriers had motor symptoms (31.7% C9orf72, 18.8% GRN, 19.3% MAPT) compared to 6.8% of controls. Slowness and gait disorder were the commonest in all genetic groups while tremor and falls were the least frequent. Symptom severity scores were similar to equivalent physical motor examination scores. PCA revealed that all motor symptoms loaded together so a single additional motor component was added to the CDR® plus NACC FTLD to form the CDR® plus NACC FTLD-M. Individual global scores were more severe with the CDR® plus NACC FTLD-M, and no patients with a clinically diagnosed motor disorder (ALS/FTD-ALS or parkinsonism) were classified anymore as asymptomatic (unlike the CDR® plus NACC FTLD alone).
Conclusions: Motor features are present in mutation carriers at all disease stages across all three genetic groups. Inclusion of motor symptoms in a rating scale that can be used in future clinical trials will not only ensure a more accurate severity measure is recorded but that a wider spectrum of FTD phenotypes can be included in the same trial.
Keywords: C9orf72; Frontotemporal dementia; Genetics; Motor; Progranulin; Tau.
© 2022. Crown.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
