

Systemic corticosteroids for the treatment of COVID-19: Equity-related analyses and update on evidence
- PMID: 36385229
- PMCID: PMC9670242
- DOI: 10.1002/14651858.CD014963.pub2
Systemic corticosteroids for the treatment of COVID-19: Equity-related analyses and update on evidence
Abstract
Background: Systemic corticosteroids are used to treat people with COVID-19 because they counter hyper-inflammation. Existing evidence syntheses suggest a slight benefit on mortality. Nonetheless, size of effect, optimal therapy regimen, and selection of patients who are likely to benefit most are factors that remain to be evaluated.
Objectives: To assess whether and at which doses systemic corticosteroids are effective and safe in the treatment of people with COVID-19, to explore equity-related aspects in subgroup analyses, and to keep up to date with the evolving evidence base using a living systematic review approach.
Search methods: We searched the Cochrane COVID-19 Study Register (which includes PubMed, Embase, CENTRAL, ClinicalTrials.gov, WHO ICTRP, and medRxiv), Web of Science (Science Citation Index, Emerging Citation Index), and the WHO COVID-19 Global literature on coronavirus disease to identify completed and ongoing studies to 6 January 2022.
Selection criteria: We included randomised controlled trials (RCTs) that evaluated systemic corticosteroids for people with COVID-19. We included any type or dose of systemic corticosteroids and the following comparisons: systemic corticosteroids plus standard care versus standard care, different types, doses and timings (early versus late) of corticosteroids. We excluded corticosteroids in combination with other active substances versus standard care, topical or inhaled corticosteroids, and corticosteroids for long-COVID treatment.
Data collection and analysis: We followed standard Cochrane methodology. To assess the risk of bias in included studies, we used the Cochrane 'Risk of bias' 2 tool for RCTs. We rated the certainty of the evidence using the GRADE approach for the following outcomes: all-cause mortality up to 30 and 120 days, discharged alive (clinical improvement), new need for invasive mechanical ventilation or death (clinical worsening), serious adverse events, adverse events, hospital-acquired infections, and invasive fungal infections.
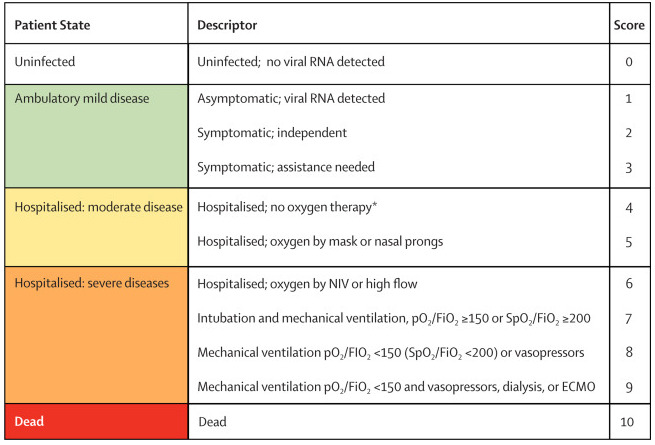
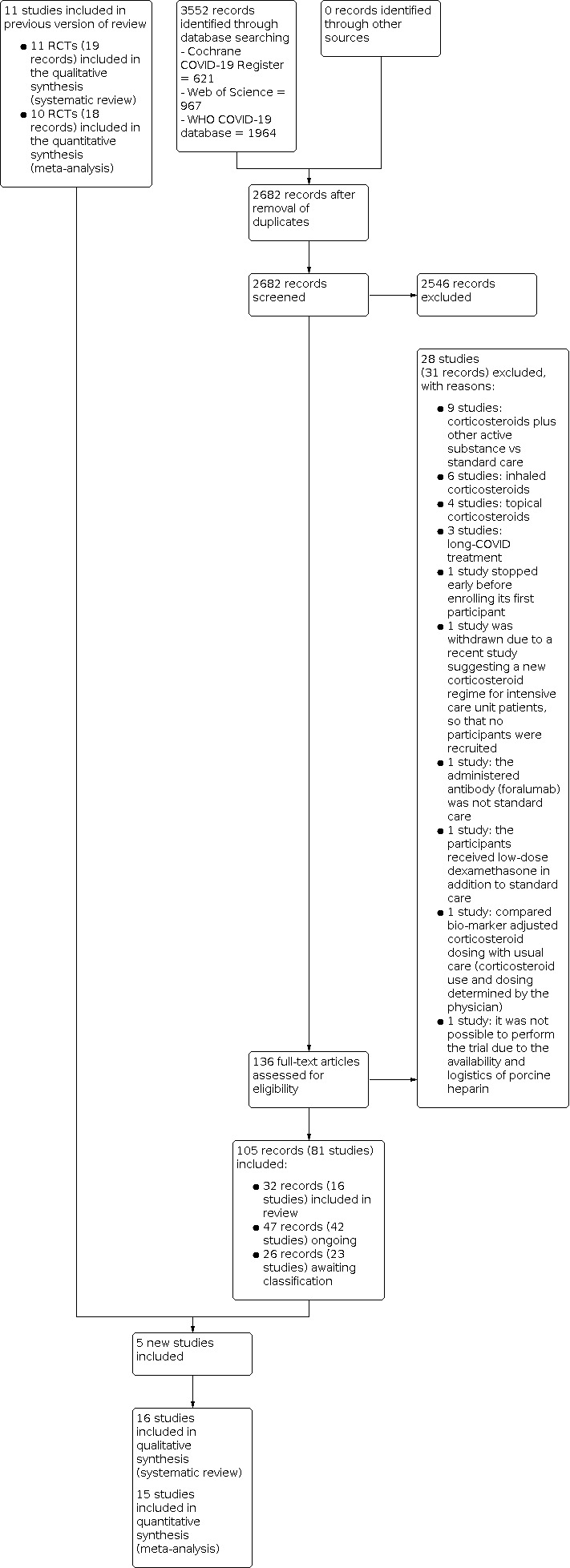
Main results: We included 16 RCTs in 9549 participants, of whom 8271 (87%) originated from high-income countries. A total of 4532 participants were randomised to corticosteroid arms and the majority received dexamethasone (n = 3766). These studies included participants mostly older than 50 years and male. We also identified 42 ongoing and 23 completed studies lacking published results or relevant information on the study design. Hospitalised individuals with a confirmed or suspected diagnosis of symptomatic COVID-19 Systemic corticosteroids plus standard care versus standard care plus/minus placebo We included 11 RCTs (8019 participants), one of which did not report any of our pre-specified outcomes and thus our analyses included outcome data from 10 studies. Systemic corticosteroids plus standard care compared to standard care probably reduce all-cause mortality (up to 30 days) slightly (risk ratio (RR) 0.90, 95% confidence interval (CI) 0.84 to 0.97; 7898 participants; estimated absolute effect: 274 deaths per 1000 people not receiving systemic corticosteroids compared to 246 deaths per 1000 people receiving the intervention (95% CI 230 to 265 per 1000 people); moderate-certainty evidence). The evidence is very uncertain about the effect on all-cause mortality (up to 120 days) (RR 0.74, 95% CI 0.23 to 2.34; 485 participants). The chance of clinical improvement (discharged alive at day 28) may slightly increase (RR 1.07, 95% CI 1.03 to 1.11; 6786 participants; low-certainty evidence) while the risk of clinical worsening (new need for invasive mechanical ventilation or death) may slightly decrease (RR 0.92, 95% CI 0.84 to 1.01; 5586 participants; low-certainty evidence). For serious adverse events (two RCTs, 678 participants), adverse events (three RCTs, 447 participants), hospital-acquired infections (four RCTs, 598 participants), and invasive fungal infections (one study, 64 participants), we did not perform any analyses beyond the presentation of descriptive statistics due to very low-certainty evidence (high risk of bias, heterogeneous definitions, and underreporting). Different types, dosages or timing of systemic corticosteroids We identified one RCT (86 participants) comparing methylprednisolone to dexamethasone, thus the evidence is very uncertain about the effect of methylprednisolone on all-cause mortality (up to 30 days) (RR 0.51, 95% CI 0.24 to 1.07; 86 participants). None of the other outcomes of interest were reported in this study. We included four RCTs (1383 participants) comparing high-dose dexamethasone (12 mg or higher) to low-dose dexamethasone (6 mg to 8 mg). High-dose dexamethasone compared to low-dose dexamethasone may reduce all-cause mortality (up to 30 days) (RR 0.87, 95% CI 0.73 to 1.04; 1269 participants; low-certainty evidence), but the evidence is very uncertain about the effect of high-dose dexamethasone on all-cause mortality (up to 120 days) (RR 0.93, 95% CI 0.79 to 1.08; 1383 participants) and it may have little or no impact on clinical improvement (discharged alive at 28 days) (RR 0.98, 95% CI 0.89 to 1.09; 200 participants; low-certainty evidence). Studies did not report data on clinical worsening (new need for invasive mechanical ventilation or death). For serious adverse events, adverse events, hospital-acquired infections, and invasive fungal infections, we did not perform analyses beyond the presentation of descriptive statistics due to very low-certainty evidence. We could not identify studies for comparisons of different timing and systemic corticosteroids versus other active substances. Equity-related subgroup analyses We conducted the following subgroup analyses to explore equity-related factors: sex, age (< 70 years; ≥ 70 years), ethnicity (Black, Asian or other versus White versus unknown) and place of residence (high-income versus low- and middle-income countries). Except for age and ethnicity, no evidence for differences could be identified. For all-cause mortality up to 30 days, participants younger than 70 years seemed to benefit from systemic corticosteroids in comparison to those aged 70 years and older. The few participants from a Black, Asian, or other minority ethnic group showed a larger estimated effect than the many White participants. Outpatients with asymptomatic or mild disease There are no studies published in populations with asymptomatic infection or mild disease.
Authors' conclusions: Systemic corticosteroids probably slightly reduce all-cause mortality up to 30 days in people hospitalised because of symptomatic COVID-19, while the evidence is very uncertain about the effect on all-cause mortality up to 120 days. For younger people (under 70 years of age) there was a potential advantage, as well as for Black, Asian, or people of a minority ethnic group; further subgroup analyses showed no relevant effects. Evidence related to the most effective type, dose, or timing of systemic corticosteroids remains immature. Currently, there is no evidence on asymptomatic or mild disease (non-hospitalised participants). Due to the low to very low certainty of the current evidence, we cannot assess safety adequately to rule out harmful effects of the treatment, therefore there is an urgent need for good-quality safety data. Findings of equity-related subgroup analyses should be interpreted with caution because of their explorative nature, low precision, and missing data. We identified 42 ongoing and 23 completed studies lacking published results or relevant information on the study design, suggesting there may be possible changes of the effect estimates and certainty of the evidence in the future.
Copyright © 2022 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
CW: Federal Ministry of Education and Research (grant/contract); staff of Cochrane Haematology.
MG: Bundesministerium für Bildung und Forschung (grant/contract); published Cochrane‐initiated Twitter posts and an upcoming Cochrane‐initiated podcast on systemic corticosteroids; Resident at the Department of Anesthesiology and Critical Care, University of Leipzig Medical Service; Member of the German Society of Anaesthesia and Intensive Care Medicine (Deutsche Gesellschaft für Anästhesiologie & Intensivmedizin, DGAI), which supports and promotes the German Clinical Practice Guideline on COVID‐19 Inpatient Therapy.
AM: no relevant interests; co‐ordination of Section COVRIIN and work in the office of STAKOB (Competence and Treatment Centres for high‐consequence infectious diseases) at Robert Koch‐Institute Centre for Biological Threats and Special Pathogens (ZBS), Section Clinical Management and Infection Control.
MIM: no relevant interests; performs editorial activities for reviews overseen by Cochrane Metabolic and Endocrine Disorders.
MSp: no relevant interests; Resident, Universitätsklinikum Leipzig.
ALF: Universitätsklinikum Leipzig AöR (employment); Fellowship in University Hospital Leipzig, 04103 Leipzig, Germany.
AAN: no relevant interests; part of Indian COVID guidelines, worked in the evidence synthesis team for inhaled steroids and HFNC versus NIV in COVID; works at the Department of Respiratory Medicine, Christian Medical College, Vellore.
JD: no relevant interests; Pulmonologist, Department of Pulmonary Medicine, CMC Vellore, India.
MS: no relevant interests; Medical Doctor, Charité – Universitätsmedizin Berlin, Germany.
NS: no relevant interests; Editor of Cochrane Haematology but was not involved in the editorial process for this review.
FF: no relevant interests; Intensive Care Consultant, University Hospital, University of Leipzig Medical Faculty.
Figures



































Update of
-
Systemic corticosteroids for the treatment of COVID-19.Cochrane Database Syst Rev. 2021 Aug 16;8(8):CD014963. doi: 10.1002/14651858.CD014963. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 Nov 17;11:CD014963. doi: 10.1002/14651858.CD014963.pub2. PMID: 34396514 Free PMC article. Updated.
References
References to studies included in this review
Angus 2020 {published data only}
-
- Angus DC, Berry S, Lewis RJ, Al-Beidh F, Arabi Y, Van Bentum-Puijk W, et al. The randomised embedded multifactorial adaptive platform for community-acquired pneumonia (REMAP-CAP) study: rationale and design. Annals of the American Thoracic Society 2020;17(7):879-91. [DOI: 10.1513/AnnalsATS.202003-192SD] - DOI - PMC - PubMed
-
- Angus DC, Derde L, Al-Beidh F, Annane D, Arabi Y, Beane A, et al. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: the REMAP-CAP COVID-19 corticosteroid domain randomised clinical trial. JAMA 2020;324(13):1317-29. [DOI: 10.1001/jama.2020.17022] [NCT02735707] - DOI - PMC - PubMed
Corral‐Gudino 2021 {published data only}
-
- Corral-Gudino L, Bahamonde A, Arnaiz-Revillas F, Gómez-Barquero J, Abadía-Otero J, García-Ibarbia C, et al. Methylprednisolone in adults hospitalised with COVID-19 pneumonia: an open-label randomised trial (GLUCOCOVID). Wiener Klinische Wochenschrift 2021;133(7-8):303-11. [DOI: 10.1007/s00508-020-01805-8] [EUCTR2020-001934-37-ES] - DOI - PMC - PubMed
-
- Corral L, Bahamonde A, Arnaiz delas Revillas F, Gomez-Barquero J, Abadia-Otero J, Garcia-Ibarbia C, et al. GLUCOCOVID: a controlled trial of methylprednisolone in adults hospitalised with COVID-19 pneumonia. medRxiv [Preprint]. [DOI: 10.1101/2020.06.17.20133579] [EUCTR2020-001934-37-ES] - DOI
Dequin 2020 {published data only}
-
- Dequin PF, Gouge AL, Tavernier E, Giraudeau B, Zohar S. Embedding a COVID-19 group sequential clinical trial within an ongoing trial: lessons from an unusual experience. Statistics in Biopharmaceutical Research 2020:1-5. [EMBASE: https://www.embase.com/search/results?subaction=viewrecord&id=L200590637...] - PMC - PubMed
-
- Dequin PF, Heming N, Meziani F, Plantefève G, Voiriot G, Badié J, et al. Effect of hydrocortisone on 21-day mortality or respiratory support among critically ill patients with COVID-19: a randomised clinical trial. JAMA 2020;324(13):1298-306. [DOI: 10.1001/jama.2020.16761] [NCT02517489] - DOI - PMC - PubMed
Edalatifard 2020 {published data only}
-
- Edalatifard M, Akhtari M, Salehi M, Naderi Z, Jamshidi A, Mostafaei S, et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: results from a randomised controlled clinical trial. European Respiratory Journal 2020;56(6):1-13. [DOI: 10.1183/13993003.02808-2020] [IRCT20200404046947N1] - DOI - PMC - PubMed
Farahani 2021 {published data only}
-
- Farahani RH, Mosaed R, Nezami-Asl A, Chamanara M, Soleiman-Meigooni S, Kalantar S, et al. Evaluation of the efficacy of methylprednisolone pulse therapy in treatment of COVID-19 adult patients with severe respiratory failure: randomised, clinical trial. Research Square 2021;Version 1:1-19. [DOI: 10.21203/rs.3.rs-66909/v1] [IRCT20200406046963N1] - DOI
Horby 2021 {published data only}
-
- Horby P, Lim WS, Emberson J, Mafham M, Bell J, Linsell L, et al. Effect of dexamethasone in hospitalised patients with COVID-19: preliminary report. medRxiv [Preprint] 2020. [DOI: ]
-
- Oxford University. Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19. University of Oxford 2020.
Jamaati 2021 {published data only}
-
- Jamaati H, Hashemian SM, Farzanegan B, Malekmohammad M, Tabarsi P, Marjani M, et al. No clinical benefit of high dose corticosteroid administration in patients with COVID-19: a preliminary report of a randomised clinical trial. European Journal of Pharmacology 2021;897:173947. [DOI: 10.1016/j.ejphar.2021.173947] [IRCT20151227025726N17] - DOI - PMC - PubMed
Jeronimo 2020 {published data only}
-
- Barros CMSS, Freire RS, Frota E, Santos AGR, Farias MAL, Rodrigues MGA, et al. Short-course of methylprednisolone improves respiratory functional parameters after 120 days in hospitalised COVID-19 patients (Metcovid Trial): a randomised clinical trial. Frontiers in Medicine 2021;8(758405):1-9. [DOI: 10.3389/fmed.2021.758405] - DOI - PMC - PubMed
-
- Jeronimo CM, Farias ME, Val FF, Sampaio VS, Alexandre MA, Melo GC, et al. Methylprednisolone as adjunctive therapy for patients hospitalised with COVID-19 (metcovid): a randomised, double-blind, phase IIb, placebo-controlled trial. Clinical Infectious Diseases 2020;72(9):e373–e81. [DOI: 10.1093/cid/ciaa1177] [NCT04343729] - DOI - PMC - PubMed
Maskin 2021 {published data only}
-
- Maskin LP, Bonelli I, Olarte GL, Palizas F Jr, Velo AE, Lurbet MF, et al. High- versus low-dose dexamethasone for the treatment of COVID-19-related acute respiratory distress syndrome: a multicenter and randomised open-label clinical trial. medRxiv 2021;Version 1:1-21. [DOI: 10.1101/2021.09.15.21263597] - DOI - PMC - PubMed
-
- Maskin LP, Bonelli I, Olarte GL, Palizas Jr F, Velo AE, Lurbet MF, et al. High- versus low-dose dexamethasone for the treatment of COVID-19-related acute respiratory distress syndrome: a multicenter, randomised open-label clinical trial. Journal of Intensive Care Medicine 2021;Version 1:1-9. [DOI: 10.1177/08850666211066799] - DOI - PMC - PubMed
-
- Maskin LP, Olarte GL, Palizas F Jr, Velo AE, Lurbet MF, Bonelli I, et al. High dose dexamethasone treatment for acute respiratory distress syndrome secondary to COVID-19: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(1):743. [DOI: 10.1186/s13063-020-04646-y] - DOI - PMC - PubMed
-
- NCT04395105. Dexamethasone for COVID-19 related ARDS: a multicenter, randomised clinical trial. clinicaltrials.gov/show/NCT04395105 (first received 20 May 2020).
Munch 2021a {published data only}
-
- Munch MW, Meyhoff TS, Helleberg M, Kjær M-BN, Granholm A, Hjortsø CJ, et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia: the COVID STEROID randomised, placebo-controlled trial. Acta Anaesthesiologica Scandinavica 2021;65(10):1421-30. [DOI: 10.1111/aas.13941] - DOI - PMC - PubMed
-
- NCT04348305. Hydrocortisone for COVID-19 and severe hypoxia. clinicaltrials.gov/show/NCT04348305 (first received 16 April 2020).
-
- Petersen MW, Meyhoff TS, Helleberg M, Nørregaard Kjær MB, Granholm A, Steensen Hjortsø CJ, et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia (COVID STEROID) trial-protocol and statistical analysis plan. Acta Anaesthesiologica Scandinavica 2020;64(9):1365-75. [DOI: 10.1111/aas.13673] - DOI - PMC - PubMed
Munch 2021b {published data only}
-
- Granholm A, Munch MW, Myatra SN, Vijayaraghavan BKT, Cronhjort M, Wahlin RR, et al. Dexamethasone 12 mg versus 6 mg for patients with COVID-19 and severe hypoxaemia: a pre-planned, secondary Bayesian analysis of the COVID STEROID 2 trial. Intensive Care Medicine 2022;48(1):45-55. [DOI: 10.1007/s00134-021-06573-1] - DOI - PMC - PubMed
Ranjbar 2021 {published data only}
-
- Ranjbar K, Shahriarirad R, Erfani A, Khodamoradi Z, Saadi MHG, et al. Methylprednisolone or dexamethasone, which one is the superior corticosteroid in the treatment of hospitalised COVID-19 patients: a triple-blinded randomised controlled trial. Research Square (Preprint). [DOI: ] [IRCT20200204046369N1]
Taboada 2021 {published data only}
-
- NCT04726098. Low or high dose of dexamethasone in patients with respiratory failure by COVID-19. clinicaltrials.gov/ct2/show/record/NCT04726098 (first received 27 January 2021).
-
- Taboada M, Rodríguez N, Varela PM, Rodríguez MT, Abelleira R, González A, et al. Effect of high versus low dose of dexamethasone on clinical worsening in patients hospitalised with moderate or severe COVID-19 pneumonia: an open-label, randomised clinical trial. European Respiratory Journal 2021;59(1):1-43. [DOI: 10.1183/13993003.02518-2021] - DOI - PMC - PubMed
Tang 2021 {published data only}
-
- Tang X, Feng YM, Ni JX, Zhang JY, Liu LM, Hu K, et al. Early use of corticosteroid may prolong SARS-CoV-2 shedding in non-intensive care unit patients with COVID-19 pneumonia: a multicenter, single-blind, randomised control trial. Respiration 2021;100(2):116-26. [DOI: 10.1159/000512063] [NCT04273321] - DOI - PMC - PubMed
Tomazini 2020 {published data only}
-
- Tomazini BM, Maia IS, Bueno FR, Silva Mvao Baldassare FP, Costa EL, Moura RA, et al. COVID-19-associated ARDS treated with dexamethasone (CoDEX): study design and rationale for a randomised trial. Revista Brasileira de Terapia Intensiva 2020;32(3):354-62. [DOI: 10.5935/0103-507X.20200063] - DOI - PMC - PubMed
-
- Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, Rosa RG, Veiga VC, et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: the CoDEX randomised clinical trial. JAMA 2020;324(13):1307-16. [DOI: 10.1001/jama.2020.17021] [NCT04327401] - DOI - PMC - PubMed
Toroghi 2021 {published data only}
-
- IRCT20100228003449N31. Corticosteroids in COVID-19. irct.ir/trial/51163 (first received 8 October 2020).
-
- Toroghi N, Abbasian L, Anahid Nourian A, Davoudi-Monfared E, Khalili H, Hasannezhad M, et al. Comparing efficacy and safety of different doses of dexamethasone in the treatment of COVID-19: a three-arm randomized clinical trial. Pharmacological Reports 2021;Version 1:1-12. [DOI: 10.1007/s43440-021-00341-0] - DOI - PMC - PubMed
References to studies excluded from this review
EUCTR2020‐001445‐39‐ES {published data only}
-
- EUCTR2020-001445-39-ES. Clinical trial to evaluate methylprednisolone pulses and tacrolimus in hospitalized patients with severe pneumonia secondary to COVID-19 (tacrovid). www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 31 March 2020).
EUCTR2020‐001616‐18‐ES {published data only}
-
- Treatment with inhaled corticoids in patients with COVID-19 and pneumonia. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2020-001616-18-ES.
EUCTR2020‐001889‐10 {published data only}
-
- EUCTR2020-001889-10. Use of inhaled corticosteroids as treatment of early COVID-19 infection to prevent clinical deterioration and hospitalisation. www.clinicaltrialsregister.eu/ctr-search/trial/2020-001889-10/GB (first received 15 May 2020).
IRCT20120225009124N4 {published data only}
-
- IRCT20120225009124N4. Letter to the editor: efficacy of different methods of combination regimen administrations including dexamethasone, intravenous immunoglobulin, and interferon-beta to treat critically ill COVID-19 patients: a structured summary of a study protocol for a randomized controlled trial. Trials 2020;21(1):549. [DOI: 10.1186/s13063-020-04499-5] - DOI - PMC - PubMed
IRCT20190312043030N2 {published data only}
-
- IRCT20190312043030N2. The effect of selenium, vitamin C and methylprednisolone combination on mortality and morbidity of COVID-19 patients. en.irct.ir/trial/49508 (first received 19 August 2020).
IRCT20200522047542N1 {published data only}
-
- IRCT20200522047542N1. Effect of corton on olfactory dysfunction in COVID-19 patients. en.irct.ir/trial/48379 (first received 4 August 2020).
ISRCTN86534580 {published data only}
-
- ISRCTN86534580. PRINCIPLE: a trial evaluating treatments for suspected COVID-19 in people aged 50 years and above with pre-existing conditions and those aged 65 years and above. www.isrctn.com/ISRCTN86534580 (first received 20 March 2020).
Moreira 2021 {published data only}
-
- Moreira TG, Matos KTF, De Paula GS, Santana TMM, Da Mata RG, Pansera FC, et al. Nasal administration of anti-CD3 monoclonal antibody (foralumab) reduces lung inflammation and blood inflammatory biomarkers in mild to moderate COVID-19 patients: a pilot study. Frontiers in Immunology 2021;12:3255. [DOI: 10.3389/fimmu.2021.709861] - DOI - PMC - PubMed
Naik 2021 {published data only}
NCT04341038 {published data only}
-
- NCT04341038. Clinical trial to evaluate methylprednisolone pulses and tacrolimus in patients with COVID-19 lung injury. clinicaltrials.gov/show/NCT04341038 (first received 10 April 2020).
-
- NCT04341038. Pragmatic, open-label, single-center, randomized, phase II clinical trial to evaluate the efficacy and safety of methylprednisolone pulses and tacrolimus in patients with severe pneumonia secondary to COVID-19: the TACROVID trial protocol. medRxiv [Preprint] 2021;21(100716):1-8. [DOI: 10.1016/j.conctc.2021.100716] - DOI - PMC - PubMed
NCT04355637 {published data only}
-
- NCT04355637. Inhaled corticosteroid treatment of COVID-19 patients with pneumonia. clinicaltrials.gov/show/NCT04355637 (first received 21 April 2020).
NCT04359511 {published data only}
-
- NCT04359511. Efficacy and safety of corticosteroids in oxygen-dependent patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04359511 (first received 24 April 2020).
NCT04361474 {published data only}
-
- Daval M, Corre A, Palpacuer C, Houssette J, Poillon G, Eliezer M, et al. Efficacy of local budesonide therapy in the management of persistent hyposmia in COVID-19 patients without signs of severity: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(666):1-3. [DOI: ] - PMC - PubMed
-
- NCT04361474. Trial evaluating the efficacy of local budesonide therapy in the management of hyposmia in COVID-19 patients without signs of severity. clinicaltrials.gov/show/NCT04361474 (first received 24 April 2020).
NCT04381364 {published data only}
-
- NCT04381364. Inhalation of ciclesonide for patients with COVID-19: a randomised open treatment study (HALT COVID-19). clinicaltrials.gov/show/NCT04381364 (first received 8 May 2020).
NCT04411667 {published data only}
NCT04416399 {published data only}
NCT04468646 {published data only}
-
- Riffat M, Fridoon A, Ahad Q, Muhammad AR, Syed AG, Muhammad AT, et al. Aprepitant as a combinant with dexamethasone reduces the inflammation via neurokinin 1 receptor antagonism in severe to critical COVID-19 patients and potentiates respiratory recovery: a novel therapeutic approach. medRxiv [Preprint]. [DOI: ]
NCT04484493 {published data only}
NCT04485429 {published data only}
-
- NCT04485429. Efficacy assessment of methylprednisolone and heparin in patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04485429 (first received 24 July 2020).
NCT04534478 {published data only}
-
- NCT04534478. Oral prednisone regimens to optimise the therapeutic strategy in patients with organising pneumonia post-COVID-19. clinicaltrials.gov/show/NCT04534478 (first received 1 September 2020).
NCT04551781 {unpublished data only}
-
- NCT04551781. Short term low dose corticosteroids for management of post COVID19 pulmonary fibrosis. clinicaltrials.gov/show/NCT04551781 (first received 16 September 2020).
NCT04561180 {published data only}
-
- NCT04561180. Study to evaluate the efficacy and safety of EG-HPCP-03a compared to DEX in patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04561180 (first received 23 September 2020).
NCT04569825 {published data only}
-
- NCT04569825. Effect of nasal steroid in the treatment of anosmia due to COVID-19 disease. clinicaltrials.gov/ct2/show/NCT04569825 (first received 30 September 2020).
NCT04640168 {published data only}
-
- NCT04640168. Adaptive COVID-19 treatment trial 4 (ACTT-4). clinicaltrials.gov/show/NCT04640168 (first received 23 November 2020).
NCT04657484 {published data only}
-
- NCT04657484. Comparison of two corticosteroid regimens for post-COVID diffuse lung disease. clinicaltrials.gov/show/NCT04657484 (first received 8 December 2020).
NCT04826822 {published data only}
-
- NCT04826822. Spironolactone and dexamethasone in patients hospitalised with COVID-19 (SPIDEX-II). clinicaltrials.gov/show/NCT04826822 (first received 1 April 2021).
NCT05133635 {published data only}
-
- NCT05133635. High-dose corticosteroid or tocilizumab for clinical worsening of COVID-19. https://clinicaltrials.gov/show/NCT05133635 (first received 11 January 2021).
References to studies awaiting assessment
EUCTR2020‐001307‐16‐ES {published data only}
-
- EUCTR2020-001307-16-ES. Efficacy and safety of corticoids in patients with adult respiratory distress syndrome (ARDS) secondary to coronavirus infection. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 1 April 2020).
EUCTR2020‐001333‐13‐FR {published data only}
-
- EUCTR2020-001333-13-FR. Dexamethasone associated with hydroxychloroquine vs. hydroxychloroquine alone for the early treatment of severe ARDS caused by COVID-19: a randomised controlled trial. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 9 April 2020).
EUCTR2020‐001553‐48‐FR {published data only}
-
- EUCTR2020-001553-48-FR. Corticoids in COVID-19 viral pneumonia in infection with SARS-CoV-2 (translation by the review authors) [Corticoides au cours de la pneumonie virale COVID-19 liee a linfection par le SARS-CoV-2]. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 13 April 2020).
EUCTR2020‐002186‐34‐ES {published data only}
-
- EUCTR2020-002186-34-ES. Efficacy of the early use of corticotherapy in CoV-2 infection to prevent the progression of acute respiratory distress syndrome (ARDS). www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 22 July 2020).
EUCTR2020‐004323‐16 {published data only}
-
- EUCTR2020-004323-16. Evaluation of the efficacy of high doses of methylprednisolone in SARS-CoV2 pneumonia patients. www.clinicaltrialsregister.eu/ctr-search/trial/2020-004323-16/IT (first received 23 November 2020).
Gautam 2021 {published data only}
-
- Gautam PB, Kumar A, Kannojia BL, Chaudhary R. A comparative study of the efficacy and outcome of methylprednisolone and dexamethasone in moderate to severe COVID-19 disease. Asian Journal of Medical Sciences 2021;12(12):17-22. [DOI: 10.3126/ajms.v12i12.39294] - DOI
Ghanei 2021 {published data only}
-
- Ghanei M, Solaymani‑Dodaran M, Qazvini A, Ghazale AH, Setarehdan SA, Saadat SH, et al. The efficacy of corticosteroids therapy in patients with moderate to severe SARS-CoV-2 infection: a multicenter, randomized, open-label trial. Respiratory Research 2021;22(245):1-14. [DOI: 10.1186/s12931-021-01833-6] - DOI - PMC - PubMed
IRCT20081027001411N3 {published data only}
-
- IRCT20081027001411N3. Effect of prednisolone on treatment of COVID-19. irct.ir/trial/46975 (first received 6 January 2020).
IRCT20120215009014N354 {published data only}
-
- IRCT20120215009014N354. Evaluating the effect of intravenous hydrocortisone, methylprednisolone, and dexamethasone in treatment of patients with moderate to severe acute respiratory distress syndrome caused by COVID-19. irct.ir/trial/48043 (first received 12 May 2020).
IRCT20160118026097N4 {published data only}
-
- IRCT20160118026097N4. The effect of dexamethasone in the treatment of high-risk COVID-19 patients. irct.ir/trial/48310 (first received 13 September 2020).
IRCT20200611047727N3 {published data only}
-
- IRCT20200611047727N3. Evaluation of efficacy and safety of low dose corticosteroid with severe pneumonia COVID-19. irct.ir/trial/49116 (first received 3 January 2021).
IRCT20201015049030N1 {published data only}
-
- IRCT20201015049030N1. Effect of dexamethasone on treatment of COVID-19. www.irct.ir/trial/51736 (first received 7 November 2020).
ISRCTN33037282 {published data only}
-
- ISRCTN33037282. Comparing two medications (dexamethasone and methylprednisolone high dose) for the treatment of pneumonia in patients with COVID-19. www.isrctn.com/ISRCTN33037282 (first received 26 November 2020).
Montalvan 2021 {published data only}
-
- Montalvan E, Carcamo B, Palacion D, Rivera S, Estevez R, Norwood D, et al. High-dose vs low-dose dexamethasone in patients with COVID-19 in a tertiary hospital in Western Honduras. Chest 2021;160(4):A1117-8. [DOI: 10.1016/j.chest.2021.07.1027] - DOI
NCT04244591 {published data only}
-
- NCT04244591. Glucocorticoid therapy for novel coronavirus critically ill patients with severe acute respiratory failure. www.clinicaltrials.gov/ct2/show/NCT04244591 (first received 28 January 2020).
NCT04325061 {published data only}
-
- NCT04325061. Efficacy of dexamethasone treatment for patients with ARDS caused by COVID-19. clinicaltrials.gov/ct2/show/NCT04325061 (first received 27 March 2020).
NCT04347980 {published data only}
-
- NCT04347980. Dexamethasone treatment for severe acute respiratory distress syndrome. clinicaltrials.gov/show/NCT04347980 (first received 15 April 2020).
NCT04438980 {published data only}
-
- Les Bujanda I, Loureiro-Amigo J, Capdevila Bastons F, Elejalde Guerra I, Anniccherico Sánchez J, Murgadella-Sancho A, et al. Treatment of COVID-19 pneumonia with glucocorticoids (CORTIVID): a structured summary of a study protocol for a randomised controlled trial. Trials 2021;22(1):43. [DOI: 10.1186/s13063-020-04999-4] - DOI - PMC - PubMed
-
- NCT04438980. Glucocorticoids in COVID-19 (CORTIVID). clinicaltrials.gov/show/NCT04438980 (first received 19 June 2020).
NCT04451174 {published data only}
-
- NCT04451174. Early use of corticosteroids in hospitalised patients with moderate COVID19 pneumonia. clinicaltrials.gov/show/NCT04451174 (first received 30 June 2020).
-
- Salinas M, Andino P, Palma L, Valencia J, Figueroa E, Ortega J. Early use of corticosteroids in non-critical patients with COVID-19 pneumonia (PREDCOVID): a structured summary of a study protocol for a randomised controlled trial. Trials 2021;22(1):92. [DOI: 10.1186/s13063-021-05046-6.] - DOI - PMC - PubMed
NCT04530409 {published data only}
-
- NCT04530409. Timing of corticosteroids in COVID-19. clinicaltrials.gov/show/NCT04530409 (first received 28 August 2020).
NCT04746430 {published data only}
-
- NCT04746430. COVID-19 primary care platform for early treatment and recovery (COPPER) study. clinicaltrials.gov/show/NCT04746430 (first received 9 February 2021).
Rashad 2021 {published data only (unpublished sought but not used)}
-
- NCT04519385. Tocilizumab versus dexamethasone in severe COVID19 cases. clinicaltrials.gov/show/NCT04519385 (first received 19 August 2020).
Salukhov 2021 {published data only}
-
- Salukhov VV, Kryukov EV, Chugunov AA, Kharitonov MA, Rudakov YV, Lakhin RE, et al. The role and place of glucocorticosteroids in treatment of COVID-19 pneumonia without hypoxemia [Роль и место глюкокортикостероидов в терапии пневмоний, вызванных COVID-19, без гипоксемии]. Meditsinskiy Sovet = Medical Council 2021;16(60):162-72. [DOI: 10.21518/2079- 701X-2021-12-162-172]
References to ongoing studies
ACTRN12621001200875 {published data only}
-
- ACTRN12621001200875. A randomised controlled trial of dexamethasone for emergency and life-threatening admissions due to COVID-19 in virtual care: the DELTA study. http://www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12621001200875 (first received 8 September 2021).
ACTRN12621001603808 {published data only}
-
- ACTRN12621001603808. The effect of prednisolone vs dexamethasone on Covid-19 in pregnancy: an open labelled randomised control trial. https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12621001603808 (first received 24 November 2021).
ChiCTR2000029386 {published data only}
-
- Qin YY, Zhou YH, Lu YQ, Sun F, Yang S, Harypursat V, et al. Effectiveness of glucocorticoid therapy in patients with severe novel coronavirus pneumonia: protocol of a randomised controlled trial. Chinese Medical Journal 2020;133(9):1080-6. [DOI: 10.1097/CM9.0000000000000791] [ChiCTR2000029386] - DOI - PMC - PubMed
ChiCTR2000029656 {published data only}
-
- ChiCTR2000029656. A randomised, open-label study to evaluate the efficacy and safety of low-dose corticosteroids in hospitalised patients with novel coronavirus pneumonia (COVID-19). www.chictr.org.cn/showprojen.aspx?proj=49086 (first received 9 February 2020).
ChiCTR2000030481 {published data only}
-
- ChiCTR2000030481. The clinical value of corticosteroid therapy timing in the treatment of novel coronavirus pneumonia (COVID-19): a prospective randomised controlled trial. www.chictr.org.cn/showprojen.aspx?proj=50453 (first received 3 March 2020).
CTRI/2020/07/026608 {published data only}
-
- CTRI/2020/07/026608. A clinical trial to study the effects of two drugs methylprednisolone and dexamethasone in patients with severe COVID-19. www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=45638 (first received 15 July 2020).
CTRI/2020/12/029894 {published data only}
-
- Comparing the effectiveness of dexamethasone versus methylprednisolone in patients with moderate COVID 19 - a randomised controlled trial. ctri.nic.in/Clinicaltrials/showallp.php?mid1=49273&EncHid=&userN... (first received 18 December 2020).
-
- CTRI/2020/12/029894. A study to compare the effectiveness of two drugs, dexamethasone versus methylprednisolone in the treatment of moderate Covid 19 patients. www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2020/12/029894.
CTRI/2020/12/030143 {published data only}
-
- CTRI/2020/12/030143. Comparison of different steroid regimes in critically ill adult patients of COVID-19. www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2020/12/030143.
-
- CTRI/2020/12/030143. Evaluation of different steroid regimes in critically ill adult patients of COVID-19 admitted to intensive care units. ctri.nic.in/Clinicaltrials/showallp.php?mid1=50886&EncHid=&userN... (first received 31 December 2020).
CTRI/2021/05/033873 {published data only}
-
- CTRI/2021/05/033873. Pre-emptive steroids to alter the disease course in COVID-19 patients. http://www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2021/05/033873 (first received: 31 May 2021).
CTRI/2021/08/035822 {published data only}
-
- CTRI/2021/08/035822. Assessment of doubling dose of dexamethasone in progressively worsening severe COVID-19 pneumonia - a randomised controlled trial. http://www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=57048 (first received 19 August 2021).
EUCTR2020‐001413‐20‐ES {published data only}
-
- EUCTR2020-001413-20-ES. Efficacy and safety of siltuximab vs. corticosteroids in hospitalized patients with COVID-19 pneumonia. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 7 April 2020).
EUCTR2020‐001457‐43‐FR {published data only}
-
- EUCTR2020-001457-43-FR. Dexamethasone and oxygen support strategies in ICU patients with COVID-19 pneumonia. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 10 April 2020).
EUCTR2020‐001622‐64‐ES {published data only}
-
- EUCTR2020-001622-64-ES. Outpatient treatment of COVID-19 with early pulmonary corticosteroids as an opportunity to modify the course of the disease. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 19 April 2020).
-
- Saiz-Rodríguez M, Peña T, Lázaro L, González A, Martínez A, Cordero JA, et al. Outpatient treatment of COVID-19 with steroids in the phase of mild pneumonia without the need for admission as an opportunity to modify the course of the disease: a structured summary of a randomised controlled trial. Trials 2020;21(632):1-3. [DOI: 10.1186/s13063-020-04575-w] - DOI - PMC - PubMed
EUCTR2020‐001707‐16‐ES {published data only}
-
- EUCTR2020-001707-16-ES. Phase III randomised, unicentric open, controlled clinical trial to demonstrate the effectiveness of tocilizumab against systemic corticotherapy in patients entered by COVID-19 with bilateral pneumonia and bad evolution. www.clinicaltrialsregister.eu/ctr-search/trial/2020-001707-16/ES (first received 25 June 2020).
EUCTR2020‐001921‐30 {published data only}
-
- Busani S, Tosi M, Mighali P, Vandelli P, D'Amico R, Marietta M, et al. Multi-centre, three arm, randomised controlled trial on the use of methylprednisolone and unfractionated heparin in critically ill ventilated patients with pneumonia from SARS-CoV-2 infection: a structured summary of a study protocol for a randomised controlled trial. Trials 2020;21(1):724. [DOI: 10.1186/s13063-020-04645-z] - DOI - PMC - PubMed
-
- EUCTR2020-001921-30. Steroids and unfractionated heparin in critically-ill patients with pneumonia from COVID-19 infection. A multicenter, interventional, randomised, three arms study design. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 26 June 2020).
EUCTR2020‐003363‐25‐DK {published data only}
-
- EUCTR2020-003363-25-DK. Higher vs. lower doses of dexamethasone in patients with COVID-19 and severe oxygen deficiency: the COVID STEROID 2 trial. www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:202... (first received 18 August 2020).
EUCTR2020‐006054‐43‐IT {published data only}
-
- EUCTR2020-006054-43-IT. Randomised controlled trial to evaluate the efficacy of per-protocol administration of methylprednisolone compared to dexamethasone in SARS-CoV-2 infections requiring respiratory support. http://www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2020-006054-43-IT (first received 22 March 2021).
EUCTR2021‐001416‐29‐ES {published data only}
-
- EUCTR2021-001416-29-ES. High-dose dexamethasone treatment for SARS-COV-2. http://www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2021-001416-29-ES (first received 26 May 2021).
EUCTR2021‐004021‐71 {published data only}
-
- EUCTR2021-004021-71. Corticosteroids for loss of smell by COVID-19 infection – COCOS trial. https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_nu... (first received 12 October 2021).
IRCT20190606043826N2 {published data only}
-
- IRCT20190606043826N2. Comparison of the effectiveness and complication of dexamethasone at doses of 8 and 24 mg in the treatment of in hospitalised patients with Covid-19. http://www.who.int/trialsearch/Trial2.aspx?TrialID=IRCT20190606043826N2 (first received 1 July 2021).
NCT04329650 {published data only}
-
- NCT04329650. Efficacy and safety of siltuximab vs. corticosteroids in hospitalised patients with COVID19 pneumonia. clinicaltrials.gov/show/NCT04329650 (first received 1 April 2020).
NCT04344730 {published data only}
-
- NCT04344730. Dexamethasone and oxygen support strategies in ICU patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04344730 (first received 14 April 2020).
NCT04345445 {published data only}
-
- NCT04345445. Study to evaluate the efficacy and safety of tocilizumab versus corticosteroids in hospitalised COVID-19 patients with high risk of progression. clinicaltrials.gov/show/NCT04345445 (first received 14 April 2020).
NCT04377503 {published data only}
-
- NCT04377503. Tocilizumab versus methylprednisolone in the cytokine release syndrome of patients with COVID-19. clinicaltrials.gov/show/NCT04377503 (first received 6 May 2020).
NCT04452565 {published data only}
-
- NCT04452565. NA-831, atazanavir and dexamethasone in the treatment of SARSCov-2 infection (NATADEX). clinicaltrials.gov/show/NCT04452565 (first received 30 June 2020).
NCT04499313 {published data only}
-
- NCT04499313. Dexamethasone versus methylprednisolone for the treatment of patients with ARDS caused by COVID-19. clinicaltrials.gov/show/NCT04499313 (first received 5 August 2020).
NCT04509973 {published data only}
-
- Munch MW, Granholm A, Myatra SN, Vijayaraghavan BK, Cronhjort M, Wahlin RR, et al. Higher vs. lower doses of dexamethasone in patients with COVID-19 and severe hypoxia (COVID STEROID 2) trial: protocol and statistical analysis plan. Acta Anaesthesiologica Scandinavica 2021;00:1-12. [DOI: 10.1111/aas.13795] - DOI - PMC - PubMed
-
- NCT04509973. Higher vs. lower doses of dexamethasone for COVID-19 and severe hypoxia. clinicaltrials.gov/show/NCT04509973 (first received 12 August 2020).
NCT04513184 {published data only}
-
- NCT04513184. Randomised clinical trial of nasal dexamethasone as an adjuvant in patients with COVID-19. clinicaltrials.gov/show/NCT04513184 (first received 14 August 2020).
NCT04528329 {published data only}
-
- NCT04528329. Anosmia and / or ageusia and early corticosteroid use. clinicaltrials.gov/show/NCT04528329 (first received 27 August 2020).
NCT04528888 {published data only}
-
- NCT04528888. Steroids and unfractionated heparin in critically ill patients with pneumonia from COVID-19 infection. clinicaltrials.gov/show/NCT04528888 (first received 27 August 2020). [EUDRA-CT: https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001921-30/IT] [NCT: https://clinicaltrials.gov/ct2/show/study/NCT04528888]
NCT04545242 {published data only}
-
- NCT04545242. Efficacy of dexamethasone in patients with acute hypoxemic respiratory failure caused by infections. clinicaltrials.gov/show/NCT04545242 (first received 10 September 2020).
NCT04636671 {published data only}
-
- NCT04636671. Methylprednisolone vs. dexamethasone in COVID-19 pneumonia (MEDEAS RCT). clinicaltrials.gov/show/NCT04636671 (first received 19 November 2020).
NCT04663555 {published data only}
-
- NCT04663555. Effect of two different doses of dexamethasone in patients with ARDS and COVID-19. clinicaltrials.gov/show/NCT04663555 (first received 11 December 2020).
NCT04673162 {published data only}
-
- NCT04673162. Evaluation of the efficacy of high doses of methylprednisolone in SARS-CoV2 (COVID-19) pneumonia patients. clinicaltrials.gov/show/NCT04673162 (first received 17 December 2020).
NCT04707534 {published data only}
-
- NCT04707534. Dexamethasone for COVID-19. clinicaltrials.gov/show/NCT04707534 (first received 13 January 2021).
NCT04765371 {published data only}
-
- NCT04765371. Comparison between prednisolone and dexamethasone on mortality in patients on oxygen therapy, with COVID-19. clinicaltrials.gov/ct2/show/NCT04765371 (first received 21 February 2021).
NCT04780581 {published data only}
-
- NCT04780581. Glucocorticoid therapy in coronavirus disease COVID-19 patients. clinicaltrials.gov/show/NCT04780581 (first received 3 March 2021).
NCT04795583 {published data only}
-
- NCT04795583. Corticosteroids for COVID-19. clinicaltrials.gov/show/NCT04795583 (first received 12 March 2021).
NCT04834375 {published data only}
-
- NCT04834375. Randomised open investigation determining steroid dose. clinicaltrials.gov/show/NCT04834375 (first received 8 April 2021).
NCT04836780 {published data only}
-
- NCT04836780. Dexamethasone early administration in hospitalised patients with COVID-19 pneumonia. clinicaltrials.gov/show/NCT04836780 (first received 8 April 2021).
NCT04860518 {published data only}
-
- NCT04860518. Human intravenous interferon beta-Ia safety and preliminary efficacy in hospitalised subjects with coronavirus (HIBISCUS). https://clinicaltrials.gov/ct2/show/NCT04860518 (first received 22 April 2021).
TCTR20211017001 {published data only}
-
- TCTR20211017001. A comparative study of the effectiveness between pulse regimen methylprednisolone versus high dose dexamethasone as the initial treatment of moderate Covid-19 pneumonia: an open-label randomised controlled trial. http://www.thaiclinicaltrials.org/show/TCTR20211017001 (first received 17 October 2021).
Additional references
Aaranjani 2021
-
- Aranjani JM, Manuel A, Abdul Razack HI, Mathew ST. COVID-19–associated mucormycosis: evidence-based critical review of an emerging infection burden during the pandemic’s second wave in India. PLOS Neglected Tropical Diseases 2021;15(11):e0009921. [DOI: 10.1371/journal.pntd.0009921] - DOI - PMC - PubMed
Ahrenfeldt 2020
Aldridge 2020
-
- Aldridge RW, Lewer D, Katikireddi SV, Mathur R, Pathak N, Burns R, et al. Black, Asian and Minority Ethnic groups in England are at increased risk of death from COVID-19: indirect standardisation of NHS mortality data. Wellcome Open Research 2020;5(88):1-20. [DOI: 10.12688/wellcomeopenres.15922.2] - DOI - PMC - PubMed
Alessi 2020
-
- Alessi J, Oliveira GB, Schaan BD, Telo GH. Dexamethasone in the era of COVID-19: friend or foe? An essay on the effects of dexamethasone and the potential risks of its inadvertent use in patients with diabetes. Diabetology and Metabolic Syndrome 2020;12(80):1-11. [DOI: 10.1186/s13098-020-00583-7] - DOI - PMC - PubMed
Allen 2017
-
- Allen L, Cobiac L, Townsend N. Quantifying the global distribution of premature mortality from non-communicable diseases. Journal of Public Health December 2017;49(4):698–703. [DOI: ] - PubMed
Ansems 2021
Aw 2007
Baqui 2020
Barnes 2006
Barros 2021
-
- Barros CMSS, Freire RS, Frota E, Santos AGR, Farias MAL, Rodrigues MGA, et al. Short-course of methylprednisolone improves respiratory functional parameters after 120 days in hospitalised COVID-19 patients (Metcovid Trial): a randomised clinical trial. Frontiers in Medicine 2021;8(758405):1-9. [DOI: 10.3389/fmed.2021.758405] - DOI - PMC - PubMed
Bhanuprasad 2021
Bourdeau 2003
-
- Bourdeau I, Stratakis CA. Glucocorticoids, Pharmacology of. In: Henry H, Norman A, editors(s). Encyclopedia of Hormones. Cambridge, MA: Academic Press, 2003:142-50. [DOI: ]
Brandal 2021
Brock 2011
Buitrago‐Garcia 2020
Caughey 2013
Chaudhuri 2021
Chen 2021
Columbia Public Health 2021
-
- Competing Risk Analysis. Columbia University Mailman School of Public Health Website. Available from www.publichealth.columbia.edu/research/population-health-methods/competi... (accessed 13 July 2021). [ACCESSED JULY 13 2021: https://www.publichealth.columbia.edu/research/population-health-methods...]
COMET 2020
-
- Core outcome set developers’ response to COVID-19. www.comet-initiative.org/Studies/Details/1538 (accessed 2 November 2020).
Deeks 2022
-
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
El‐Kebbi 2021
EMA 2022
-
- European Medicines Agency (EMA). COVID-19 treatments. Available at: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-thr... (accessed 12 December 2021).
FDA 2022
-
- FDA US Food & Drug Administration. Coronavirus Disease 2019 (COVID-19). Available at: https://www.fda.gov/emergency-preparedness-and-response/counterterrorism... (accessed 12 December 2021). - PubMed
Ferguson 2021
-
- Ferguson N, Ghani A, Hinsley W, Volz E. Hospitalisation risk for Omicron cases in England. Imperial College London 2021;www.gov.uk:1-12. [DOI: 10.25561/93035] - DOI
Funk 2021
-
- Funk T, Pharris A, Spiteri G, Bundle N, Melidou A, Carr M, et al. Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance 2021;26(16):2100348. [DOI: 10.2807/1560-7917.ES.2021.26.16.2100348] - DOI - PMC - PubMed
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), accessed 18 July 2021. Available at gradepro.org.
Griesel 2022
Higgins 2003
Higgins 2019
-
- Higgins JP, Savovic J, Page MJ, Sterne JA. Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). www.riskofbias.info/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed 7 July 2021).
Higgins 2022
-
- Higgins JP, Lasserson T, Chandler J, Tovey D, Thomas J, Flemyng E, et al. Methodological expectations of Cochrane intervention reviews. www.community.cochrane.org/mecir-manual/ (accessed 6 January 2022).
Higgins 2022a
-
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from: training.cochrane.org/handbook 2022.
Higgins 2022b
-
- Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
Higgins 2022c
-
- Higgins J, Eldridge S, Li T. Chapter 23: Including variants on randomised trials. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 202s). Cochrane, 2022. Available from training.cochrane.org/handbook.
Higgins 2022d
-
- Higgins JP, Li T, Deeks JJ, editor(s). Chapter 6: Choosing effect measures and computing estimates of effect. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
Hoenigl 2022
Huang 2020
Johns Hopkins University 2022
-
- Johns Hopkins University. Mortality analyses. coronavirus.jhu.edu/data/mortality (accessed 4 April 2022).
Kluge 2022
-
- Kluge S, Janssens U, Welte T, Weber-Carstens S, Schälte G, Spinner CD, et al. S3 Guideline – recommendations for inpatient therapy of patients with COVID-19 [S3-Leitlinie – Empfehlungen zur stationären Therapie von Patienten mit COVID-19]. www.awmf.org/uploads/tx_szleitlinien/113-001LGl_S3_Empfehlungen-zur-stat... (accessed 7 April 2022). - PubMed
Kreuzberger 2021
Lauer 2020
Lewnard 2022
Li 2021
-
- Li T, Higgins JP, Deeks JJ (editors). Chapter 5: Collecting data. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 6.1 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Liang 2020
Liu 2021
Living Evidence Network 2019
-
- Living Evidence Network. Guidance for the production and publication of Cochrane living systematic reviews: Cochrane Reviews in living mode (Version December 2019). Available from community.cochrane.org/review-production/production-resources/living-sys... (accessed 22 March 2021).
Marshall 2020
Mathur 2021
-
- Mathur R, Rentsch CT, Morton CE, Hulme WJ, Schultze A, MacKenna B, et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. Lancet 2021;397(10286):1711-24. [DOI: 10.1016/S0140-6736(21)00634-6] - DOI - PMC - PubMed
Microsoft 2018 [Computer program]
-
- Microsoft Excel. Microsoft Corporation. Microsoft Corporation, 2018. office.microsoft.com/excel.
Mikolajewska 2021
Moher 2009
-
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Journal of Clinical Epidemiology 2009;62(10):1006-12. - PubMed
Morales 2021
Navar 2021
NICE 2021
-
- NICE. COVID-19 rapid guideline: managing COVID-19. https://www.nice.org.uk/guidance/ng191/resources/covid19-rapid-guideline....
NIH 2021
-
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines.nih.gov/. - PubMed
Oke 2020
-
- Oke J, Heneghan C. Global Covid-19 case fatality rates. https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/ (accessed 17 August 2022).
Oran 2020
Ouzzani 2016
Park 2020
Parmar 1998
-
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815-34. - PubMed
Pasin 2021
-
- Pasin L, Navalesi P, Zangrillo A, Kuzovlev A, Likhvantsev V, Hajjar LA, et al. Corticosteroids for patients with coronavirus disease 2019 (COVID-19) with different disease severity: a meta-analysis of randomized clinical trials. Journal of Cardiothoracic and Vascular Anesthesia 2021;35(2):578-84. [DOI: ] - PMC - PubMed
Piechotta 2021
-
- Piechotta V, Iannizzi C, Chai KL, Valk SJ, Kimber C, Dorando E, et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID‐19: a living systematic review. Cochrane Database of Systematic Reviews 2021, Issue 5. Art. No: CD013600. [DOI: 10.1002/14651858.CD013600.pub4] - DOI - PMC - PubMed
Potere 2020
-
- Potere N, Valeriani E, Candeloro M, Tana M, Porreca E, Abbate A, et al. A higher mortality rate and long ventilation times differentiate COVID-19 from severe respiratory infections in flu waves [Eine höhere Letalität und lange Beatmungsdauer unterscheiden COVID-19 von schwer verlaufenden Atemwegsinfektionen in Grippewellen]. Critical Care 2020;24(1):389. [DOI: 10.25646/7111] - DOI - PMC - PubMed
Prakash 2019
Ramachandran 2012
Ramanan 2022
RevMan Web 2019 [Computer program]
-
- Review Manager Web (RevMan Web). The Cochrane Collaboration, 2019. revman.cochrane.org.
Rhen 2005
Rochwerg 2018
-
- Rochwerg B, Oczkowski SJ, Siemieniuk RA, Agoritsas T, Belley-Cote E, D'Aragon F, et al. Corticosteroids in sepsis: an updated systematic review and meta-analysis. Critical Care Medicine 2018;46(9):1411-20. [PMID: ] - PubMed
Santesso 2020
-
- Santesso N, Glenton C, Dahm P, Garner P, Akl A, Alper B, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. Journal of Clinical Epidemiology 2020;119:126-35. - PubMed
Schreiber 2014
Schulte‐Schrepping 2020
Schünemann 2021
-
- Schünemann HJ, Higgins JP, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.
Siemieniuk 2020
-
- Siemieniuk RA, Bartoszko JJ, Ge L, Zeraatkar D, Izcovich A, Kum E, et al. Drug treatments for COVID-19: living systematic review and network meta-analysis. BMJ 2020;370:m2980. [BMJ: https://www.bmj.com/content/370/bmj.m2980] - PMC - PubMed
Skoetz 2020
-
- Skoetz N, Goldkuhle M, Van Dalen EC, Akl EA, Trivella M, Mustafa RA, et al. GRADE guidelines 27: how to calculate absolute effects for time-to-event outcomes in summary of findings tables and evidence profiles. Journal of Clinical Epidemiology 2020;118:124-31. - PubMed
Sterne 2019
-
- Sterne JA, Savovic J, Page MJ, Elbers RG, Blencowe N, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. - PubMed
Sterne 2020
Stoelting 2006
-
- Stoelting RK, Hiller SC (editors). Pharmacology. In: Pharmacology & Physiology in Anesthetic Practice. 4 edition. Philadelphia: Lippincott Williams & Wilkins, 2006:462.
Struyf 2020
-
- Struyf T, Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Leeflang MM, et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database of Systematic Reviews 2020, Issue 7. Art. No: CD013665. [DOI: 10.1002/14651858.CD013665] - DOI - PMC - PubMed
Taves 2011
Thibeault 2021
-
- Thibeault C, Mühlemann B, Helbig ET, Mittermaier M, Lingscheid T, Tober-Lau P, et al. Clinical and virological characteristics of hospitalised COVID-19 patients in a German tertiary care centre during the first wave of the SARS-CoV-2 pandemic: a prospective observational study. Infection 2021;49(4):703-14. - PMC - PubMed
Tierney 2007
Tomlinson 2021
Van Paassen 2020
Villar 2020
-
- Villar J, Ferrando C, Martínez D, Ambrós A, Muñoz T, Soler JA, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respiratory Medicine 2020;8(3):267-76. - PubMed
Waljee 2017
Wan 2021
Watson 2022
Welch 2012
WHO 2007
-
- World Health Organization. Cumulative number of reported probable cases of SARS. www.who.int/csr/sars/country/2003_07_11/en (accessed 22 March 2021).
WHO 2019
-
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). www.who.int/emergencies/mers-cov/en (accessed 22 March 2021).
WHO 2020a
-
- World Health Organization. Report of the WHO‐China joint mission on coronavirus disease 2019 (COVID‐19). www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-... (accessed 22 March 2021).
WHO 2020b
-
- World Health Organization. Estimating mortality from COVID-19 - scientific brief. www.who.int/publications/i/item/WHO-2019-nCoV-Sci-Brief-Mortality-2020.1 (accessed 22 March 2021).
WHO 2020c
WHO 2021a
-
- World Health Organization. Weekly epidemiological update - 23 February 2021. www.who.int/publications/m/item/weekly-epidemiological-update---23-febru... (accessed 1 March 2021).
WHO 2021b
-
- World Health Organization. Therapeutics and COVID-19: living guideline. 6 July 2021. 6. Who do the recommendations apply to? www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1.
WHO 2021c
-
- WHO. Therapeutics and COVID-19: living guideline. 6 July 2021. 7. Recommendations for therapeutics. 7.6 Systemic corticosteroids (published 2 September 2020). www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2021.2.
WHO 2022a
-
- World Health Organization. WHO coronavirus disease (COVID-19) dashboard. covid19.who.int (accessed 31 March 2022).
WHO 2022b
-
- World Health Organization. SARS-CoV-2 variants. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed 4 April 2022). - PubMed
Williamson 2020
Wolter 2022
World Bank 2021
-
- World Bank Country and Lending Groups. datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-coun... (accessed 15 April 2021). [WEBSITE: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-b...]
Wu 2020
Yasir 2022
-
- Yasir M, Goyal A, Sonthalia S. Corticosteroid adverse effects. StatPearls Publishing 2022. [https://www.ncbi.nlm.nih.gov/books/NBK531462/] - PubMed
References to other published versions of this review
Wagner 2021a
Wagner 2021b
-
- Wagner C, Griesel M, Micholajewska A, Fichtner F, Skoetz N. Corticosteroids for the treatment of COVID-19 (part of German Ecosystem CEO-Sys). PROSPERO 1 February 2021 (available from www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=227450). [PROSPERO: CRD42020227450]
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources