

T cells specific for α-myosin drive immunotherapy-related myocarditis
- PMID: 36385524
- PMCID: PMC9930174
- DOI: 10.1038/s41586-022-05432-3
T cells specific for α-myosin drive immunotherapy-related myocarditis
Abstract
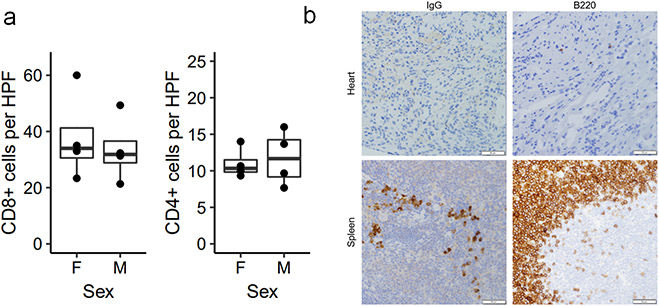
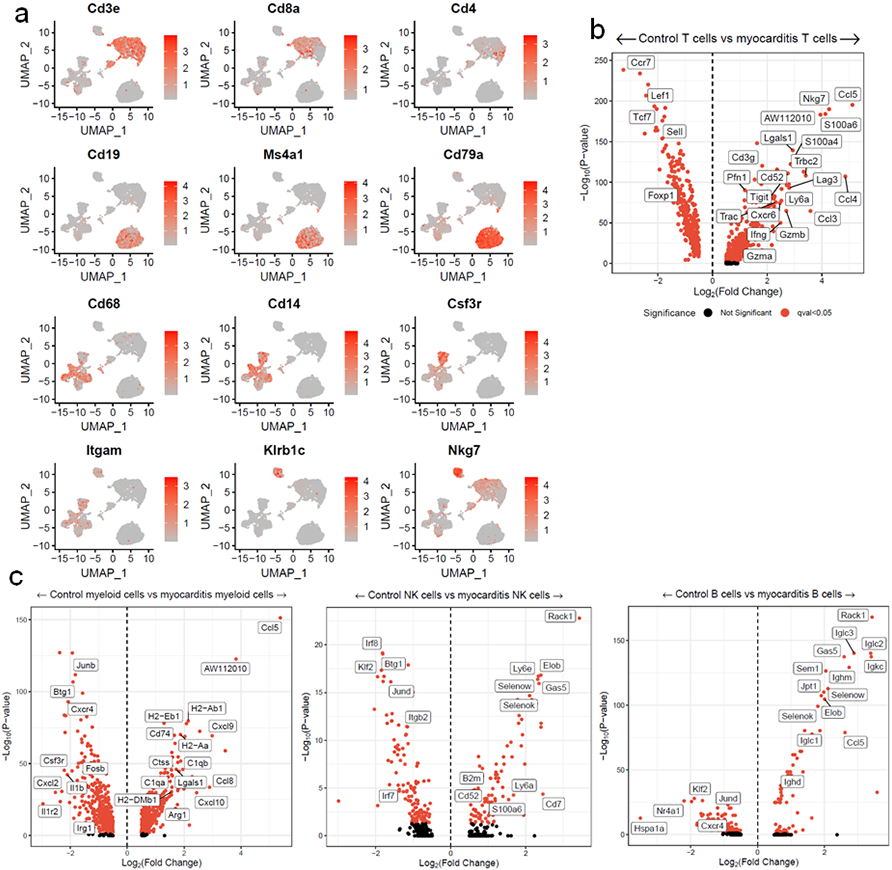
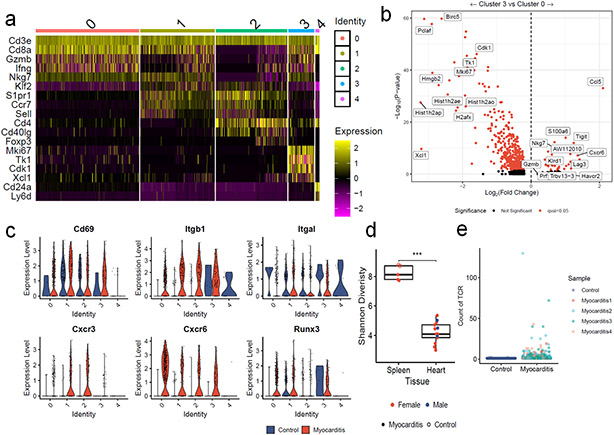
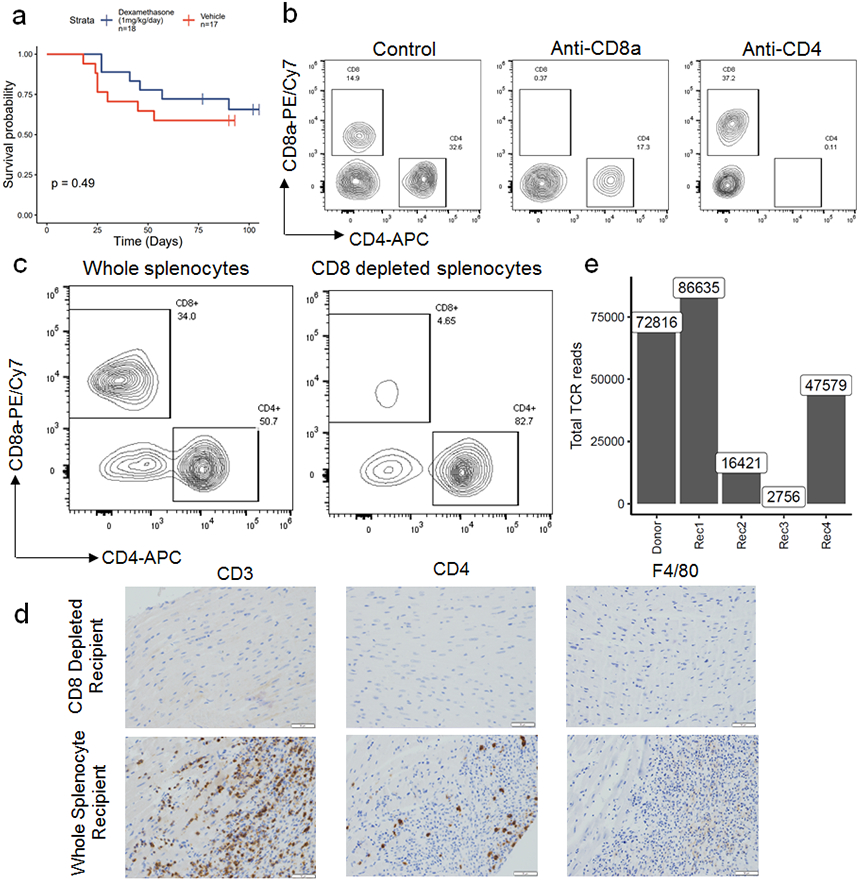
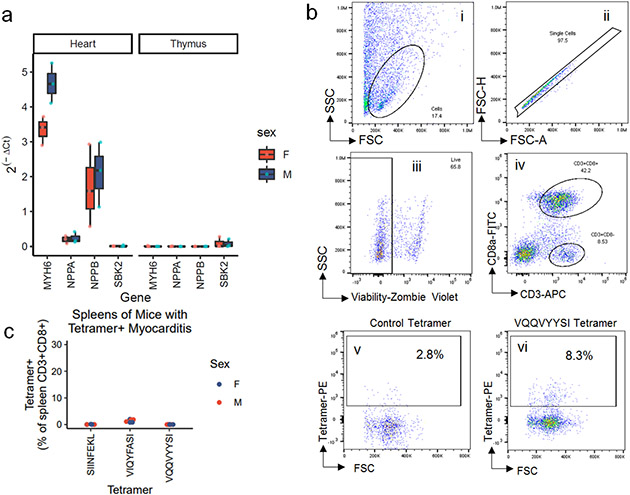
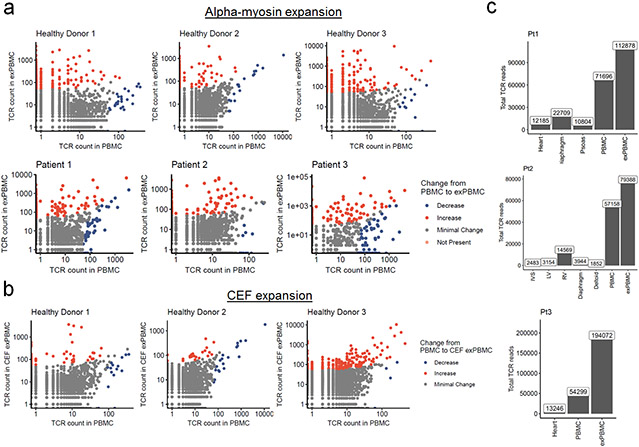
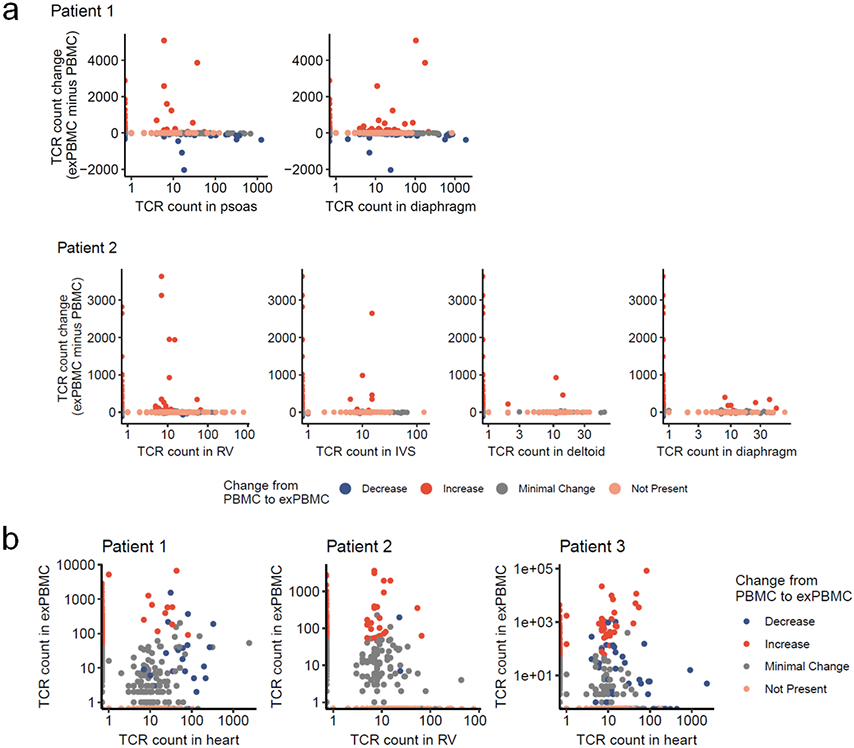
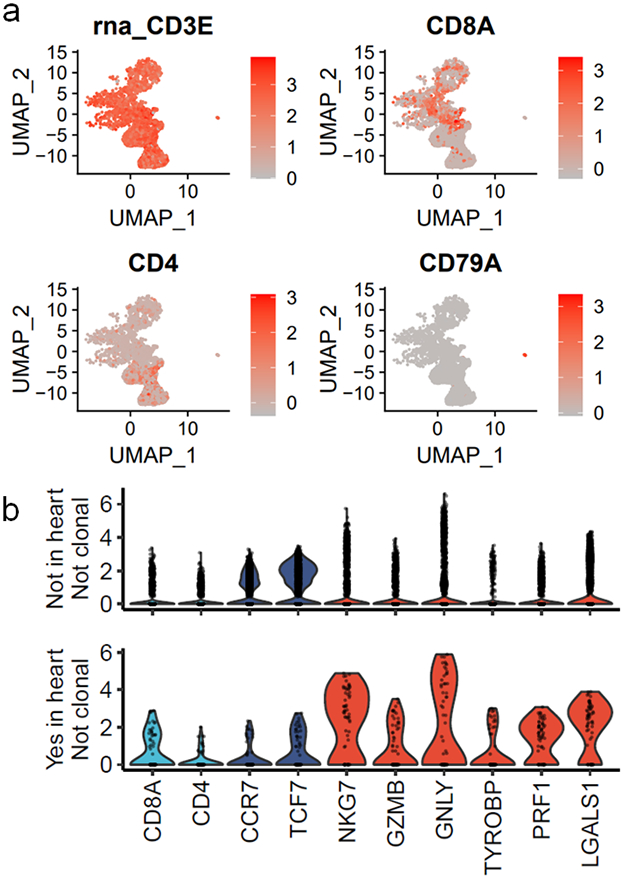
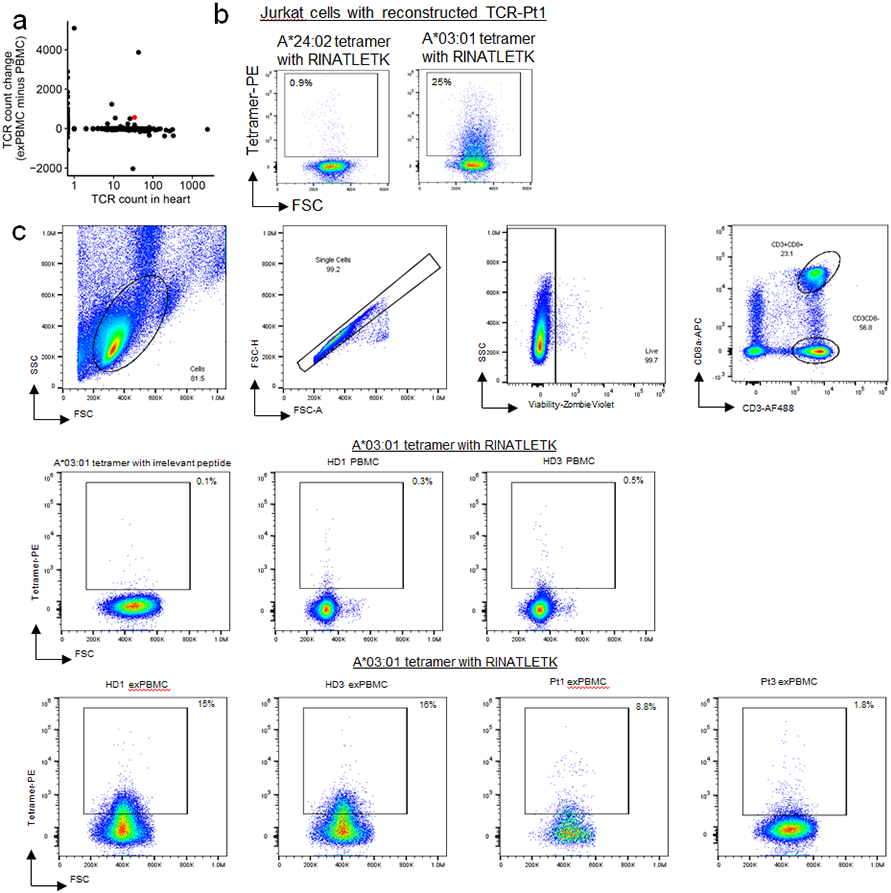
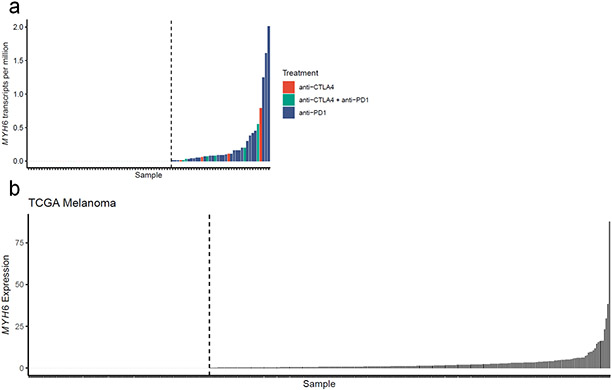
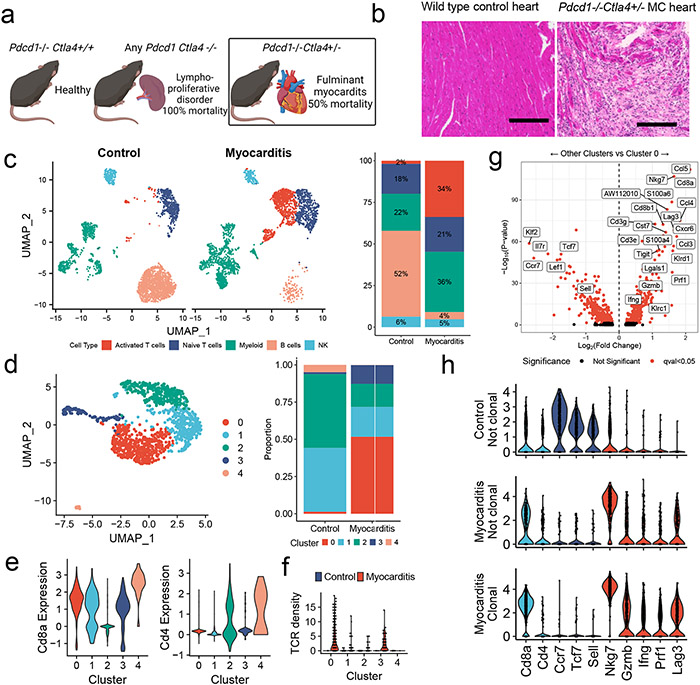
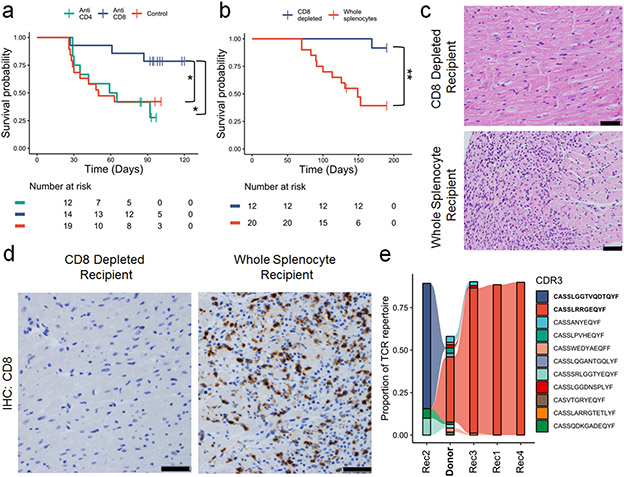
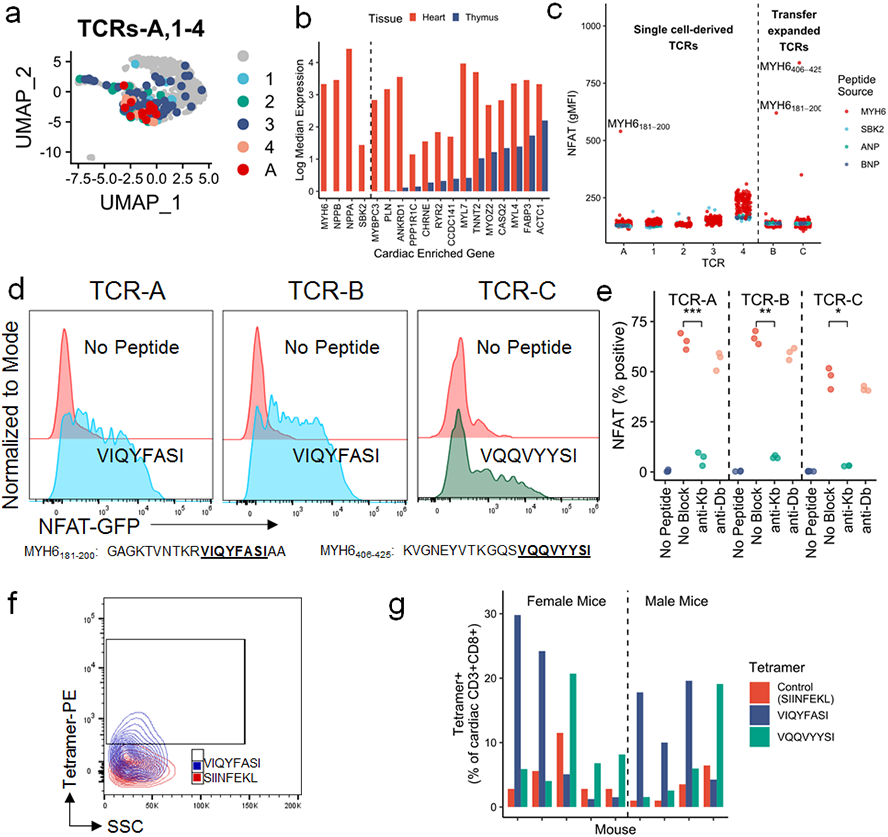
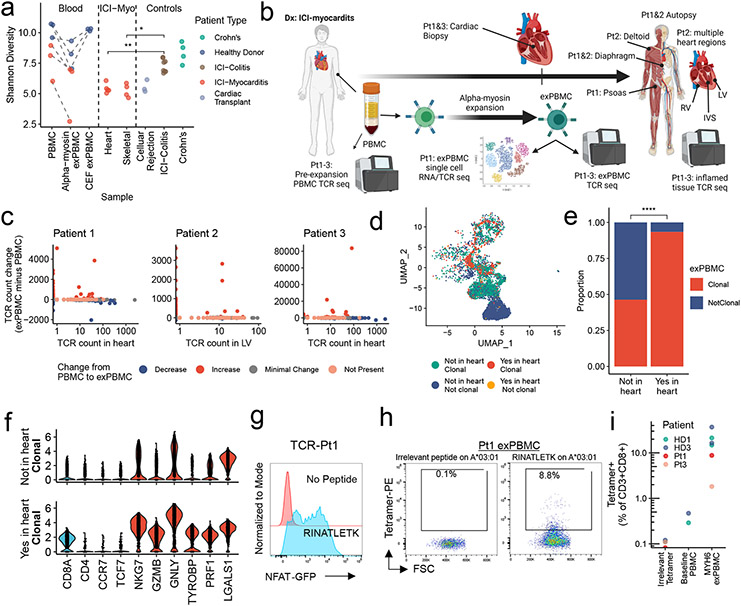
Immune-related adverse events, particularly severe toxicities such as myocarditis, are major challenges to the utility of immune checkpoint inhibitors (ICIs) in anticancer therapy1. The pathogenesis of ICI-associated myocarditis (ICI-MC) is poorly understood. Pdcd1-/-Ctla4+/- mice recapitulate clinicopathological features of ICI-MC, including myocardial T cell infiltration2. Here, using single-cell RNA and T cell receptor (TCR) sequencing of cardiac immune infiltrates from Pdcd1-/-Ctla4+/- mice, we identify clonal effector CD8+ T cells as the dominant cell population. Treatment with anti-CD8-depleting, but not anti-CD4-depleting, antibodies improved the survival of Pdcd1-/-Ctla4+/- mice. Adoptive transfer of immune cells from mice with myocarditis induced fatal myocarditis in recipients, which required CD8+ T cells. The cardiac-specific protein α-myosin, which is absent from the thymus3,4, was identified as the cognate antigen source for three major histocompatibility complex class I-restricted TCRs derived from mice with fulminant myocarditis. Peripheral blood T cells from three patients with ICI-MC were expanded by α-myosin peptides. Moreover, these α-myosin-expanded T cells shared TCR clonotypes with diseased heart and skeletal muscle, which indicates that α-myosin may be a clinically important autoantigen in ICI-MC. These studies underscore the crucial role for cytotoxic CD8+ T cells, identify a candidate autoantigen in ICI-MC and yield new insights into the pathogenesis of ICI toxicity.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Conflict of Interest Disclosure
M.L. Axelrod is listed as a coinventor on a provisional patent application for methods to predict therapeutic outcomes using blood-based gene expression patterns, that is owned by Vanderbilt University Medical Center, and is currently unlicensed. S.C. Wei is an employee of Spotlight Therapeutics, a consultant for BioEntre, and an inventor on a patent for a genetic mouse model of autoimmune adverse events and immune checkpoint blockade therapy (PCT/US2019/050551) pending to Board of Regents, The University of Texas System. K. Amancherla serves on the Data Safety Monitoring Board for ACI Clinical. J.C. Rathmell is a founder, scientific advisory board member, and stockholder of Sitryx Therapeutics, a scientific advisory board member and stockholder of Caribou Biosciences, a member of the scientific advisory board of Nirogy Therapeutics, has consulted for Merck, Pfizer, and Mitobridge within the past three years, and has received research support from Incyte Corp., Calithera Biosciences, and Tempest Therapeutics. P.B. Ferrell receives research support from Incyte Corporation. D.B.Johnson has served on advisory boards or as a consultant for BMS, Catalyst Biopharma, Iovance, Jansen, Mallinckrodt, Merck, Mosaic ImmunoEngineering, Novartis, Oncosec, Pfizer, and Targovax, has received research funding from BMS and Incyte, and has patents pending for use of MHC-II as a biomarker for immune checkpoint inhibitor response, and abatacept as treatment for immune-related adverse events. J.P. Allison reports personal fees from Achelois, Adaptive Biotechnologies, personal fees from Apricity Health, personal fees from BioAtla, Candel Therapeutics, personal fees from Codiak BioSciences, personal fees from Dragonfly Therapeutics, Earli, Enable Medicine, personal fees from Hummingbird, personal fees from ImaginAb, personal fees from Jounce Therapeutics, personal fees from Lava Therapeutics, personal fees from Lytix Biopharma, personal fees from Marker Therapeutics, PBM Capital, Phenomic AI, personal fees from BioNTech, and personal fees from Polaris Pharma, Time Bioventures, Trained Therapeutics, Two Bear Capital, Venn Biosciences outside the submitted work; in addition, J.P. Allison has a patent for a genetic mouse model of immune checkpoint blockade induced immune-related adverse events pending to The University of Texas MD Anderson Cancer Center; and have received royalties from intellectual property licensed to BMS and Merck. J. Moslehi has served on advisory boards for Bristol Myers Squibb, Takeda, Audentes, Deciphera, Janssen, Immuno-Core, Boston Biomedical, Amgen, Myovant, Kurome Therapeutics, Star Therapeutics, ProtinQure, Pharmacyclics, Pfizer, Mallinckrodt Pharmaceuticals, Silverback Therapeutics, Cytokinetics, and AstraZeneca. J. M. Balko receives research support from Genentech/Roche, and Incyte Corporation, and is an inventor on provisional patents regarding immunotherapy targets and biomarkers in cancer. No disclosures were reported by the other authors.
Figures
Comment in
-
α-Myosin-specific CD8+ T cells drive ICI-related myocarditis.Nat Rev Cardiol. 2023 Feb;20(2):75. doi: 10.1038/s41569-022-00821-7. Nat Rev Cardiol. 2023. PMID: 36450928 No abstract available.
-
The potential of auto-antigen-guided treatment of immune checkpoint inhibitor-mediated myocarditis.Med. 2023 Jan 13;4(1):13-14. doi: 10.1016/j.medj.2022.12.005. Med. 2023. PMID: 36640753
References
-
- Wang DY, Salem J-EE, Cohen JV., et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018;4(12):1721–1728. http://www.embase.com/search/results?subaction=viewrecord&from=export&id.... Accessed October 15, 2019. - PMC - PubMed
-
- Wei SC, Meijers WC, Axelrod ML, et al. A Genetic Mouse Model Recapitulates Immune Checkpoint Inhibitor–Associated Myocarditis and Supports a Mechanism-Based Therapeutic Intervention. Cancer Discov. 2020;11(3):614–639. doi:10.1158/2159-8290.cd-20-0856 - DOI - PMC - PubMed
Methods only extended references
Publication types
MeSH terms
Substances
Grants and funding
- T32 DK007061/DK/NIDDK NIH HHS/United States
- S10 OD023475/OD/NIH HHS/United States
- R01 HL156021/HL/NHLBI NIH HHS/United States
- R01 HL141466/HL/NHLBI NIH HHS/United States
- F30 CA236157/CA/NCI NIH HHS/United States
- T32 HL007895/HL/NHLBI NIH HHS/United States
- G20 RR030956/RR/NCRR NIH HHS/United States
- R01 AI152183/AI/NIAID NIH HHS/United States
- T32 GM007347/GM/NIGMS NIH HHS/United States
- AHA/American Heart Association-American Stroke Association/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- R01 CA217987/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- R01 HG010863/HG/NHGRI NIH HHS/United States
- S10 OD025092/OD/NIH HHS/United States
- P30 EY008126/EY/NEI NIH HHS/United States
- R01 CA227481/CA/NCI NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- P30 AI110527/AI/NIAID NIH HHS/United States
- R01 HL155990/HL/NHLBI NIH HHS/United States
- K23 HL138291/HL/NHLBI NIH HHS/United States
- U01 AI154659/AI/NIAID NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
