

Dementia risk after major elective surgery based on the route of anaesthesia: A propensity score-matched population-based cohort study
- PMID: 36386032
- PMCID: PMC9641180
- DOI: 10.1016/j.eclinm.2022.101727
Dementia risk after major elective surgery based on the route of anaesthesia: A propensity score-matched population-based cohort study
Abstract
Background: Whether the route of anaesthesia is an independent risk factor for dementia remains unclear. Therefore, we conducted a propensity score-matched (PSM) population-based cohort study to compare dementia incidence among surgical patients undergoing different routes of anaesthesia.
Methods: The inclusion criteria were being an inpatient >20 years of age who underwent major elective surgery, defined as those requiring GA without or with inhalation anaesthetics or regional anaesthesia, and being hospitalised for >1 day between Jan 1, 2008 and Dec 31, 2019 in Taiwan. Patients undergoing major elective surgery were categorised into three groups according to the type of anaesthesia administered: noninhalation anaesthesia, inhalation anaesthesia, and regional anaesthesia, matched at a 1:1 ratio. The incidence rate (IR) of dementia was determined.
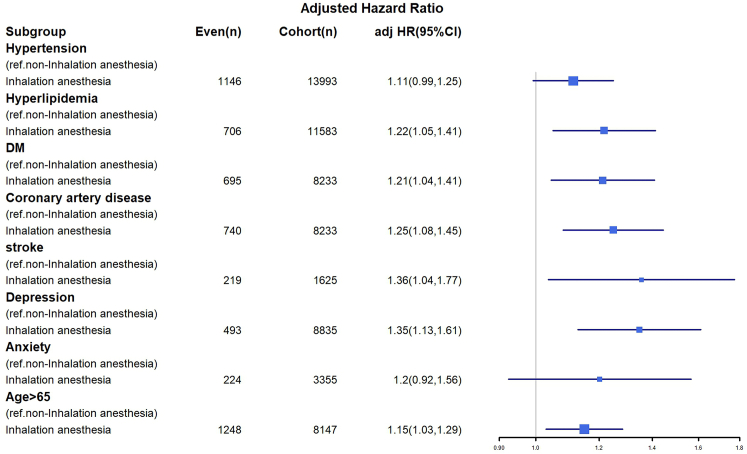
Findings: PSM yielded 63,750 patients (21,250 in the noninhalation anaesthesia group, 21,250 in the inhalation anaesthesia group, and 21,250 in the regional anaesthesia group). In the multivariate Cox regression analysis, the adjusted hazard ratios (aHRs; 95% confidence intervals) of dementia for the inhalation and noninhalation anaesthesia groups compared with the regional anaesthesia group were 20.16 (15.40-26.35; p < 0.001) and 18.33 (14.03-24.04; p < 0.001), respectively. The aHR of dementia for inhalation anaesthesia compared with noninhalation anaesthesia was 1.13 (1.03-1.22; p = 0.028). The IRs of dementia for the inhalation, noninhalation, and regional anaesthesia groups were 3647.90, 3492.00, and 272.99 per 100,000 person-years, respectively.
Interpretation: In this population based cohort study, the incidence of dementia among surgical patients undergoing general anaesthesia was higher than among those undergoing regional anaesthesia. Among patients undergoing general anaesthesia, inhalation anaesthesia was associated with a higher risk of dementia than noninhalation anaesthesia. Our results should be confirmed in a randomised controlled trial.
Funding: The study was partially supported by Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital (Funding Number: 10908, 10909, 11001, 11002, 11003, 11006, and 11013).
Keywords: AD, Alzheimer disease; ASA, American Society of Anesthesiology; Anaesthesia; CI, confidence interval; Dementia; GA, General anaesthesia; General anaesthesia; HR, hazard ratio; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; IPTW, inverse probability of treatment weighting; IQR, interquartile range; IRRs, incidence rate ratios; IRs, incidence rates; Incidence rate; NHIRD, National Health Insurance Research Database; PSM, propensity score matching; RCT, randomised controlled trial; Regional anaesthesia; SD, standard deviation; SMD, standardized mean difference; aHR, adjusted hazard ratio.
© 2022 The Author(s).
Conflict of interest statement
The authors have no potential conflicts of interest to declare.
Figures

References
-
- Xu J., Zhang Y., Qiu C., Cheng F. Global and regional economic costs of dementia: a systematic review. Lancet. 2017;390:S47.
-
- World Health Organization . Regional Office for the Eastern Mediterranean; 2019. Dementia: World Health Organization.
-
- Moller J.T., Cluitmans P., Rasmussen L.S., et al. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet. 1998;351(9106):857–861. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
