

Prevalence of left ventricular hypertrophy in children and young people with primary hypertension: Meta-analysis and meta-regression
- PMID: 36386367
- PMCID: PMC9659762
- DOI: 10.3389/fcvm.2022.993513
Prevalence of left ventricular hypertrophy in children and young people with primary hypertension: Meta-analysis and meta-regression
Abstract
Background: Left ventricular hypertrophy (LVH) is the main marker of HMOD in children and young people (CYP). We aimed to assess the prevalence of LVH and its determinants in CYP with primary hypertension (PH).
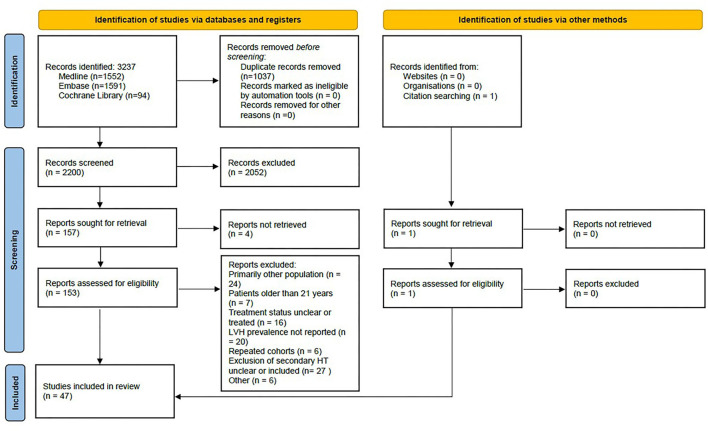
Methods: A meta-analysis of prevalence was performed. A literature search of articles reporting LVH in CYP with PH was conducted in Medline, Embase, and Cochrane databases. Studies with a primary focus on CYP (up to 21 years) with PH were included. Meta-regression was used to analyze factors explaining observed heterogeneity.
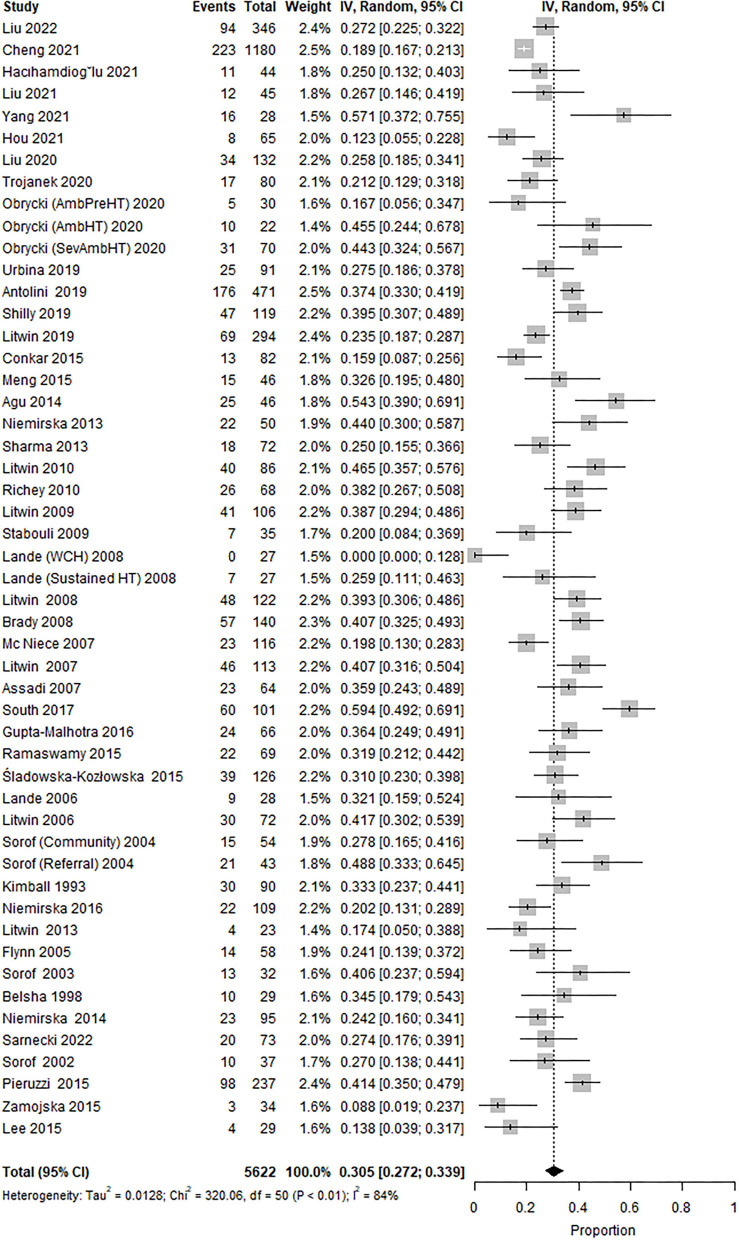
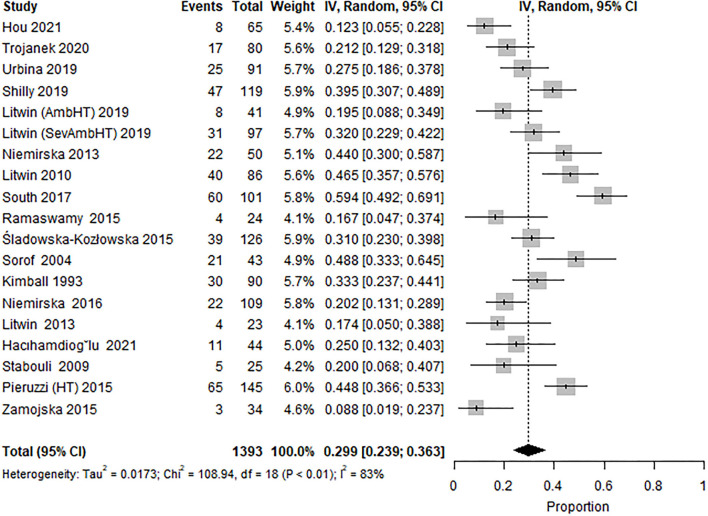
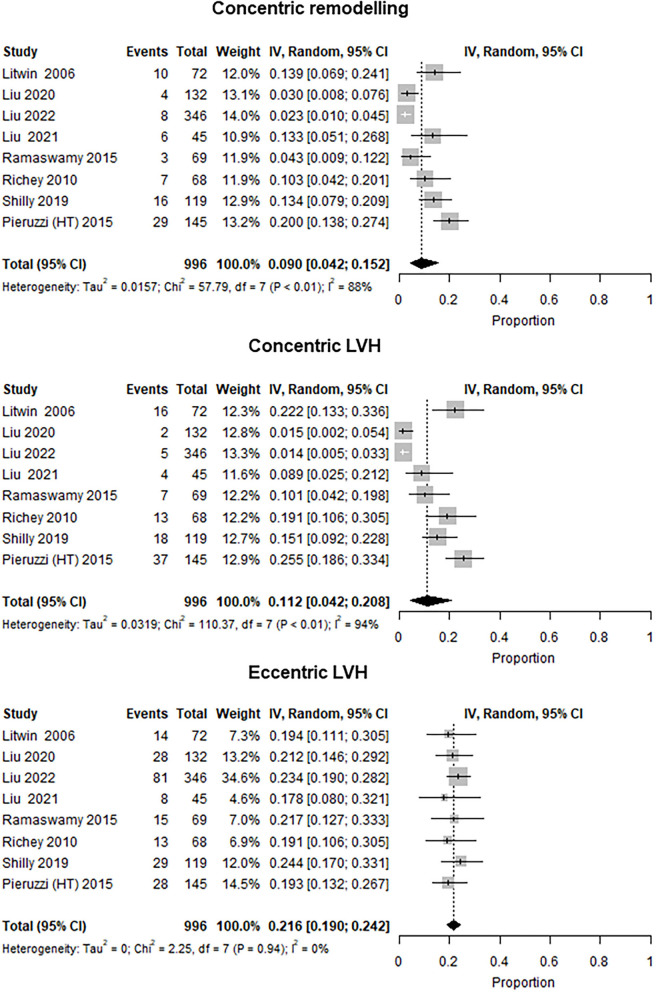
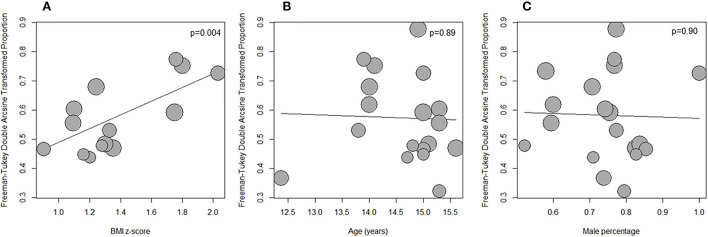
Results: The search yielded a total of 2,200 articles, 153 of those underwent full-text review, and 47 reports were included. The reports evaluated 51 study cohorts including 5,622 individuals, 73% male subjects, and a mean age of 13.6 years. LVH was defined as left ventricle mass index (LVMI) ≥ 95th percentile in 22 (47%), fixed cut-off ≥38.6 g/m2.7 in eight (17%), sex-specific fixed cut-off values in six (13%), and miscellaneously in others. The overall prevalence of LVH was 30.5% (95% CI 27.2-33.9), while heterogeneity was high (I 2 = 84%). Subgroup analysis including 1,393 individuals (76% male subjects, mean age 14.7 years) from pediatric hypertension specialty clinics and LVH defined as LVMI ≥95th percentile only (19 study cohorts from 18 studies), reported prevalence of LVH at 29.9% (95% CI 23.9 to 36.3), and high heterogeneity (I 2 = 84%). Two studies involving patients identified through community screening (n = 1,234) reported lower LVH prevalence (21.5%). In the meta-regression, only body mass index (BMI) z-score was significantly associated with LVH prevalence (estimate 0.23, 95% CI 0.08-0.39, p = 0.004) and accounted for 41% of observed heterogeneity, but not age, male percentage, BMI, or waist circumference z-score. The predominant LVH phenotype was eccentric LVH in patients from specialty clinics (prevalence of 22% in seven studies with 779 participants) and one community screening study reported the predominance of concentric LVH (12%).
Conclusion: Left ventricular hypertrophy is evident in at least one-fifth of children and young adults with PH and in nearly a third of those referred to specialty clinics with a predominant eccentric LVH pattern in the latter. Increased BMI is the most significant risk association for LVH in hypertensive youth.
Keywords: adolescents; children; left ventricular hypertrophy; left ventricular mass index; primary hypertension.
Copyright © 2022 Sinha, Azukaitis, Sladowska-Kozłowska, Bårdsen, Merkevicius, Karlsen Sletten, Obrycki, Pac, Fernández-Aranda, Bjelakovic, Jankauskiene, Litwin and HyperChildNet Working Group.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. (2021) 398:957–80. 10.1016/S0140-6736(21)01330-1 - DOI - PMC - PubMed