

Remotely delivered cognitive behavioural and personalised exercise interventions for fatigue severity and impact in inflammatory rheumatic diseases (LIFT): a multicentre, randomised, controlled, open-label, parallel-group trial
- PMID: 36388001
- PMCID: PMC9646481
- DOI: 10.1016/S2665-9913(22)00156-4
Remotely delivered cognitive behavioural and personalised exercise interventions for fatigue severity and impact in inflammatory rheumatic diseases (LIFT): a multicentre, randomised, controlled, open-label, parallel-group trial
Abstract
Background: Chronic fatigue is a poorly managed problem in people with inflammatory rheumatic diseases. Cognitive behavioural approaches (CBA) and personalised exercise programmes (PEP) can be effective, but they are not often implemented because their effectivenesses across the different inflammatory rheumatic diseases are unknown and regular face-to-face sessions are often undesirable, especially during a pandemic. We hypothesised that remotely delivered CBA and PEP would effectively alleviate fatigue severity and life impact across inflammatory rheumatic diseases.
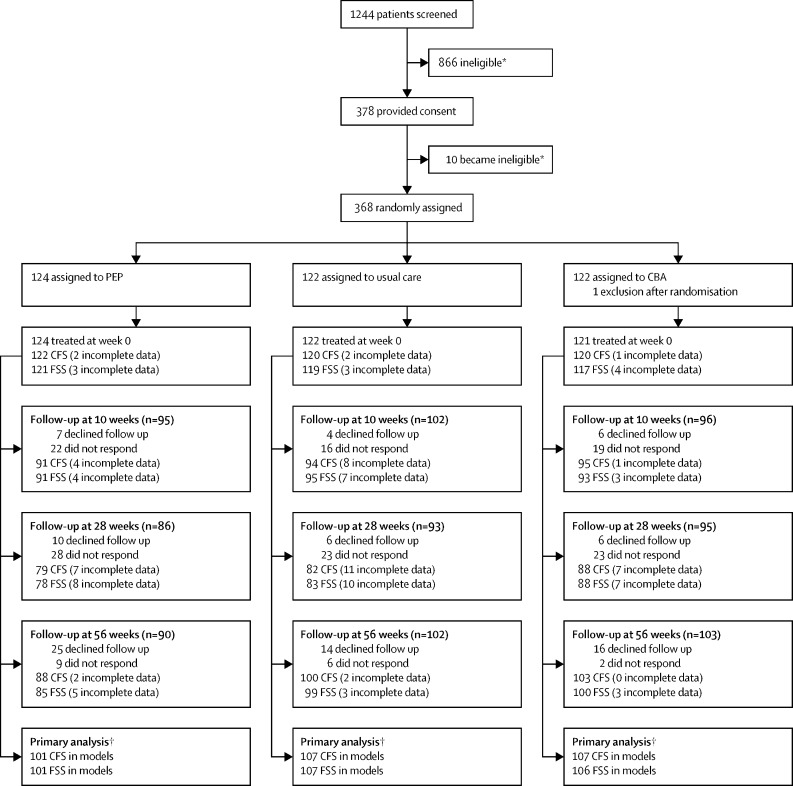
Methods: LIFT is a multicentre, randomised, controlled, open-label, parallel-group trial to assess usual care alongside telephone-delivered CBA or PEP against usual care alone in UK hospitals. Patients with any stable inflammatory rheumatic disease were eligible if they reported clinically significant, persistent fatigue. Treatment allocation was assigned by a web-based randomisation system. CBA and PEP sessions were delivered over 6 months by trained health professionals in rheumatology. Coprimary outcomes were fatigue severity (Chalder Fatigue Scale) and impact (Fatigue Severity Scale) at 56 weeks. The primary analysis was by full analysis set. This study was registered at ClinicalTrials.gov (NCT03248518).
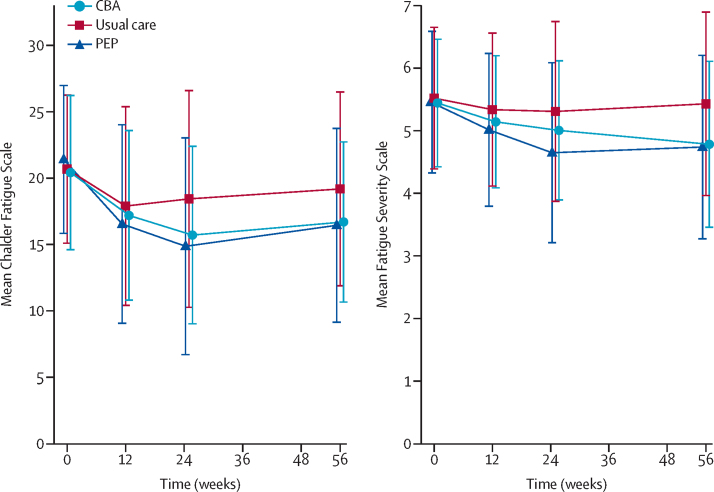
Findings: From Sept 4, 2017, to Sept 30, 2019, we randomly assigned and treated 367 participants to PEP (n=124; one participant withdrew after being randomly assinged), CBA (n=121), or usual care alone (n=122), of whom 274 (75%) were women and 92 (25%) were men with an overall mean age of 57·5 (SD 12·7) years. Analyses for Chalder Fatigue Scale included 101 participants in the PEP group, 107 in the CBA group, and 107 in the usual care group and for Fatigue Severity Scale included 101 in PEP, 106 in CBA, and 107 in usual care groups. PEP and CBA significantly improved fatigue severity (Chalder Fatigue Scale; PEP: adjusted mean difference -3·03 [97·5% CI -5·05 to -1·02], p=0·0007; CBA: -2·36 [-4·28 to -0·44], p=0·0058) and fatigue impact (Fatigue Severity Scale; PEP: -0·64 [-0·95 to -0·33], p<0·0001; CBA: -0·58 [-0·87 to -0·28], p<0·0001); compared with usual care alone at 56 weeks. No trial-related serious adverse events were reported.
Interpretation: Telephone-delivered CBA and PEP produced and maintained statistically and clinically significant reductions in the severity and impact of fatigue in a variety of inflammatory rheumatic diseases. These interventions should be considered as a key component of inflammatory rheumatic disease management in routine clinical practice.
Funding: Versus Arthritis.
© 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Conflict of interest statement
We declare no competing interests.
Figures
Similar articles
-
Protocol for a multicentre randomised controlled parallel-group trial to compare the effectiveness of remotely delivered cognitive-behavioural and graded exercise interventions with usual care alone to lessen the impact of fatigue in inflammatory rheumatic diseases (LIFT).BMJ Open. 2019 Jan 30;9(1):e026793. doi: 10.1136/bmjopen-2018-026793. BMJ Open. 2019. PMID: 30705244 Free PMC article.
-
Group cognitive-behavioural programme to reduce the impact of rheumatoid arthritis fatigue: the RAFT RCT with economic and qualitative evaluations.Health Technol Assess. 2019 Oct;23(57):1-130. doi: 10.3310/hta23570. Health Technol Assess. 2019. PMID: 31601357 Free PMC article. Clinical Trial.
-
Cost-effectiveness of cognitive behavioural and personalized exercise interventions for reducing fatigue in inflammatory rheumatic diseases.Rheumatology (Oxford). 2023 Dec 1;62(12):3819-3827. doi: 10.1093/rheumatology/kead157. Rheumatology (Oxford). 2023. PMID: 37018151 Free PMC article. Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
Cited by
-
Efficacy of a cognitive-behavioral digital therapeutic on psychosocial outcomes in rheumatoid arthritis: randomized controlled trial.Npj Ment Health Res. 2024 Sep 3;3(1):41. doi: 10.1038/s44184-024-00085-8. Npj Ment Health Res. 2024. PMID: 39227501 Free PMC article.
-
Impact of fatigue on work productivity and health-related job loss.Occup Med (Lond). 2024 Sep 23;74(6):423-429. doi: 10.1093/occmed/kqae056. Occup Med (Lond). 2024. PMID: 38970820 Free PMC article.
-
Impaired health-related quality of life in idiopathic inflammatory myopathies: a cross-sectional analysis from the COVAD-2 e-survey.Rheumatol Adv Pract. 2024 Mar 4;8(2):rkae028. doi: 10.1093/rap/rkae028. eCollection 2024. Rheumatol Adv Pract. 2024. PMID: 38524696 Free PMC article.
-
Fatigue levels and associated factors in systemic sclerosis: a cross-sectional study of 2385 SPIN Cohort participants.Rheumatology (Oxford). 2025 May 1;64(5):2810-2820. doi: 10.1093/rheumatology/keae570. Rheumatology (Oxford). 2025. PMID: 39447026 Free PMC article.
-
Patients with rheumatoid arthritis presenting with mono- or oligo-arthritis and high VAS-ratings remain the most fatigued during 5 years of follow-up.Rheumatology (Oxford). 2024 May 3;63(6):1574-1581. doi: 10.1093/rheumatology/kead429. Rheumatology (Oxford). 2024. PMID: 37632771 Free PMC article.
References
-
- Smith E, Hoy DG, Cross M, et al. The global burden of other musculoskeletal disorders: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73:1462–1469. - PubMed
-
- Repping-Wuts H, van Riel P, van Achterberg T. Fatigue in patients with rheumatoid arthritis: what is known and what is needed. Rheumatology (Oxford) 2009;48:207–209. - PubMed
-
- van Hoogmoed D, Fransen J, Bleijenberg G, van Riel P. Physical and psychosocial correlates of severe fatigue in rheumatoid arthritis. Rheumatology (Oxford) 2010;49:1294–1302. - PubMed
-
- Dures E, Cramp F, Hackett K, Primdahl J. Fatigue in inflammatory arthritis. Best Pract Res Clin Rheumatol. 2020;34 - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
