

Multisuture and Syndromic Craniosynostoses: Simplifying the Complex
- PMID: 36388010
- PMCID: PMC9648657
- DOI: 10.4103/jpn.JPN_26_22
Multisuture and Syndromic Craniosynostoses: Simplifying the Complex
Abstract
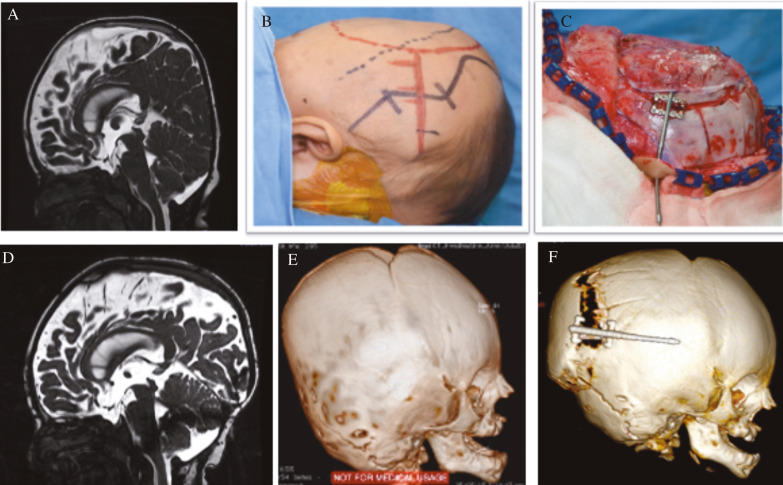
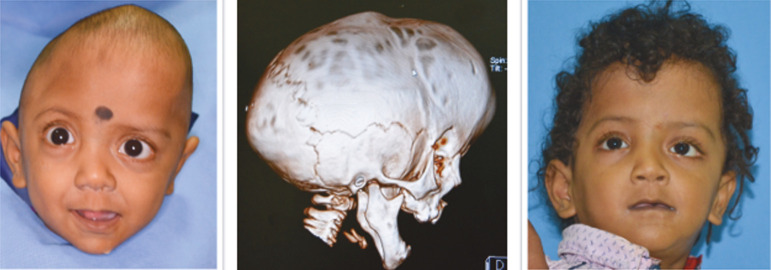
Most complex craniosynostoses are managed the same way as syndromic craniosynostoses (SCs), as these patients often experience similar problems regarding cognition and increased intracranial pressure (ICP). The evaluation and treatment plan for craniosynostoses is complex, and this, additionally, is complicated by the age at presentation. In this article, the authors review the complexity of SCs in the presentation and management. An algorithm is necessary for such multifaceted and multidimensional pathology as craniosynostoses. In most algorithms, posterior calvarial distraction is a consistent early option for complex craniosynostoses presenting early with raised ICP. Addressing the airway early is critical when significant airway issues are there. All other surgical interventions are tailored on the basis of presentation and age.
Keywords: Algorithm; complex; craniosynostoses; management; multisutural; syndromic.
Copyright: © 2022 Journal of Pediatric Neurosciences.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures







References
-
- Tolarova MM, Harris JA, Ordway DE, Vargervik K. Birth prevalence, mutation rate, sex ratio, parents’ age, and ethnicity in Apert syndrome. Am J Med Genet. 1997;72:394–8. - PubMed
-
- Armand T, Schaefer E, Di Rocco F, Edery P, Collet C, Rossi M. Genetic bases of craniosynostoses: An update. Neurochirurgie. 2019;65:196–201. - PubMed
-
- Di Rocco F, Rothenbuhler A, Cormier Daire V, Bacchetta J, Adamsbaum C, Baujat G, et al. Craniosynostosis and metabolic bone disorder. A review. Neurochirurgie. 2019;65:258–63. - PubMed
-
- Kalmar CL, Zapatero ZD, Kosyk MS, Carlson AR, Bartlett SP, Heuer GG, et al. Elevated intracranial pressure with craniosynostosis: A multivariate model of age, syndromic status, and number of involved cranial sutures. J Neurosurg Pediatr. 2021;28:1–8. - PubMed
-
- Jabs EW, Müller U, Li X, Ma L, Luo W, Haworth IS, et al. A mutation in the homeodomain of the human Msx2 gene in a family affected with autosomal dominant craniosynostosis. Cell. 1993;75:443–50. - PubMed
Publication types
LinkOut - more resources
Full Text Sources