

Reversing painful and non-painful diabetic neuropathy with the capsaicin 8% patch: Clinical evidence for pain relief and restoration of function via nerve fiber regeneration
- PMID: 36388188
- PMCID: PMC9643187
- DOI: 10.3389/fneur.2022.998904
Reversing painful and non-painful diabetic neuropathy with the capsaicin 8% patch: Clinical evidence for pain relief and restoration of function via nerve fiber regeneration
Abstract
Introduction: Current oral treatments for pain in diabetic peripheral neuropathy (DPN) do not affect the progression of DPN i.e., "disease modification." We assessed whether Capsaicin 8% patch treatment can provide pain relief and also restore nerve density and function via nerve regeneration, in both painful (PDPN) and non-painful (NPDPN) diabetic peripheral neuropathy.
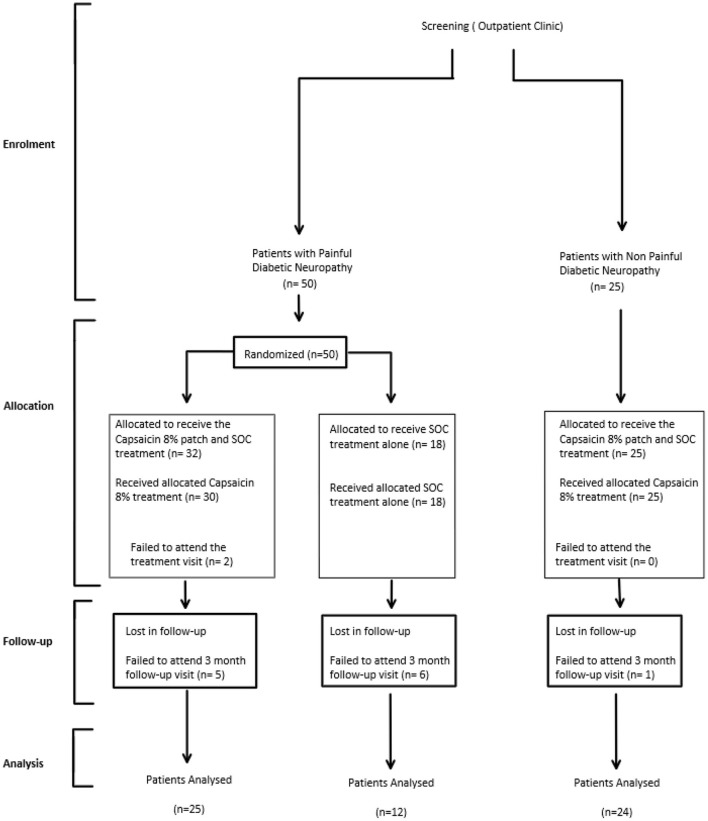
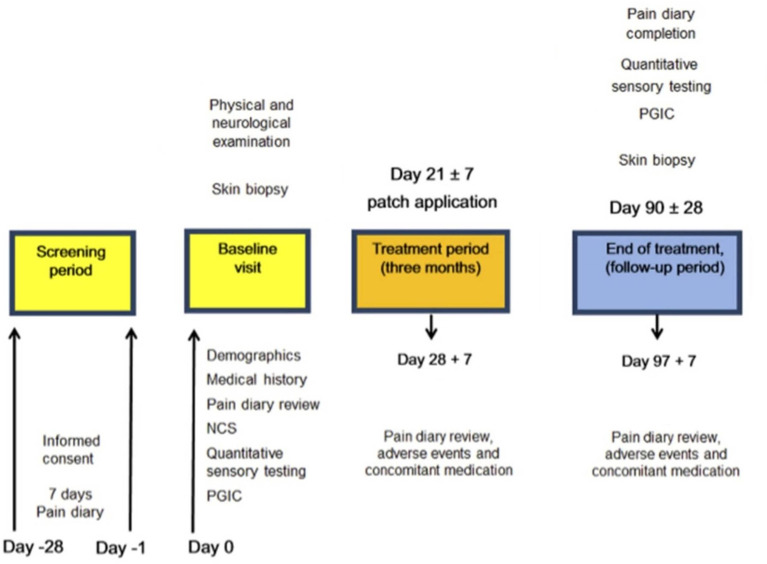
Methods: 50 participants with PDPN were randomized to receive Capsaicin 8% patch Qutenza with Standard of Care (SOC) (PDPN Q+SOC group), or SOC alone (PDPN SOC group). Pain symptoms were assessed with a diary (Numerical Pain Rating Scale, NRPS) and questionnaires. Investigations included quantitative sensory testing (QST) and distal calf skin biopsies, at baseline and 3 months after baseline visit; subsequent options were 3-monthly visits over 1 year. 25 participants with NPDPN had tests at baseline, and 3 months after all received Capsaicin 8% patch treatment.
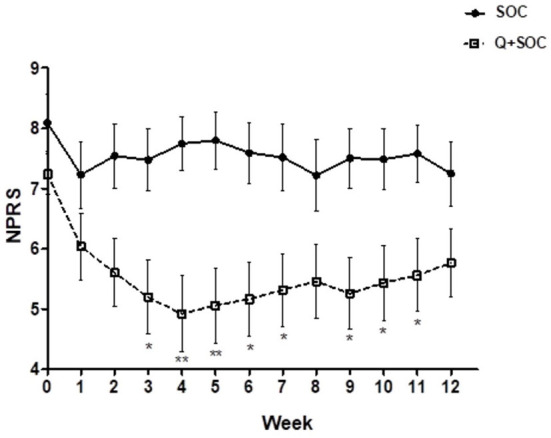
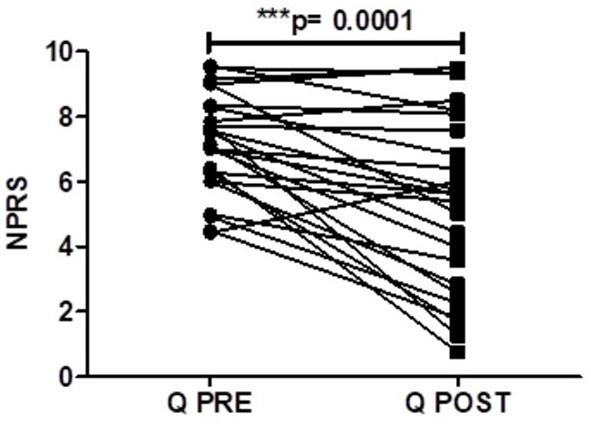
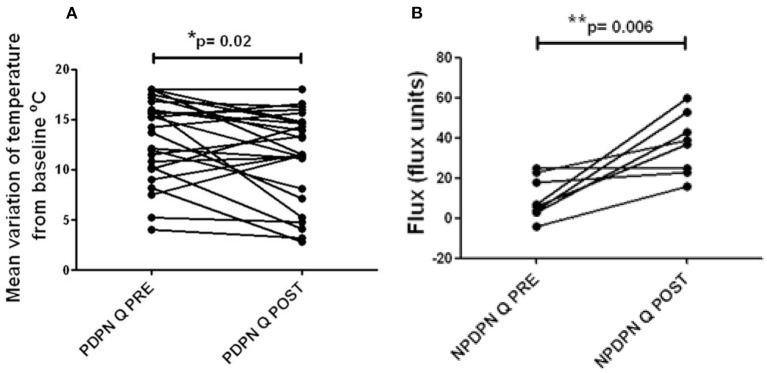
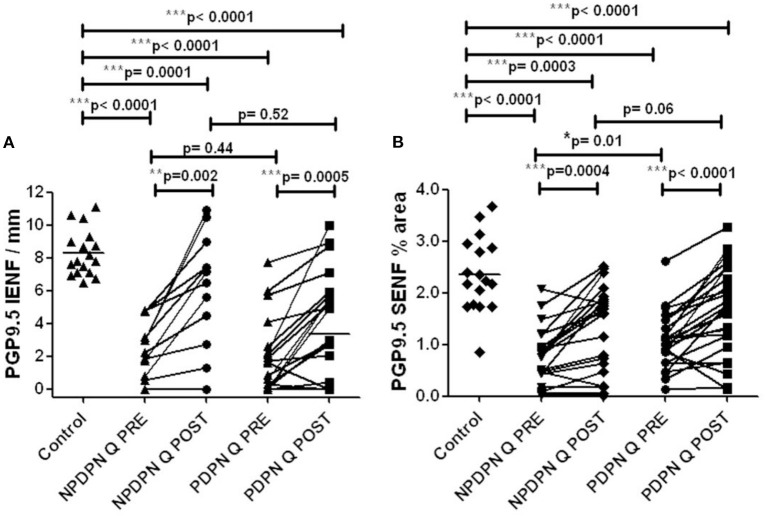
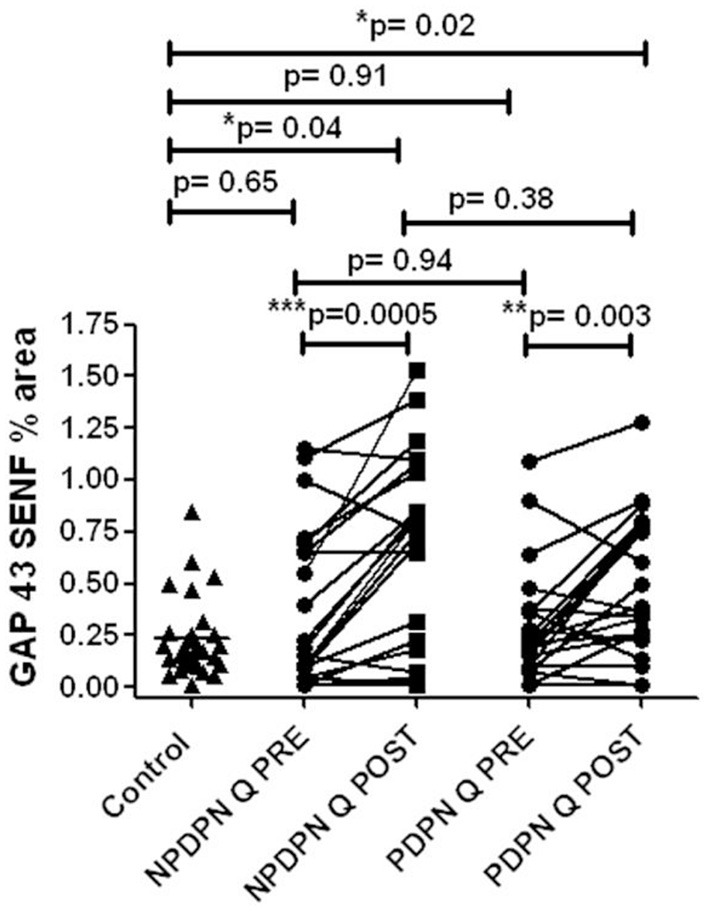
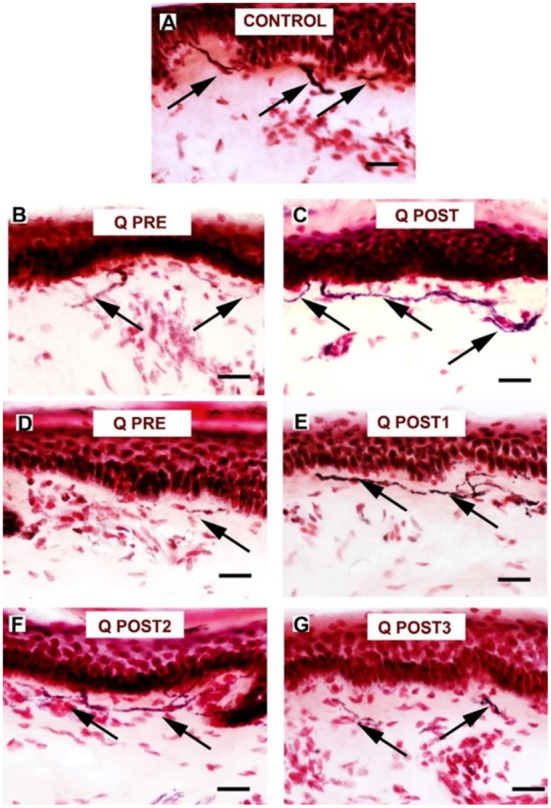
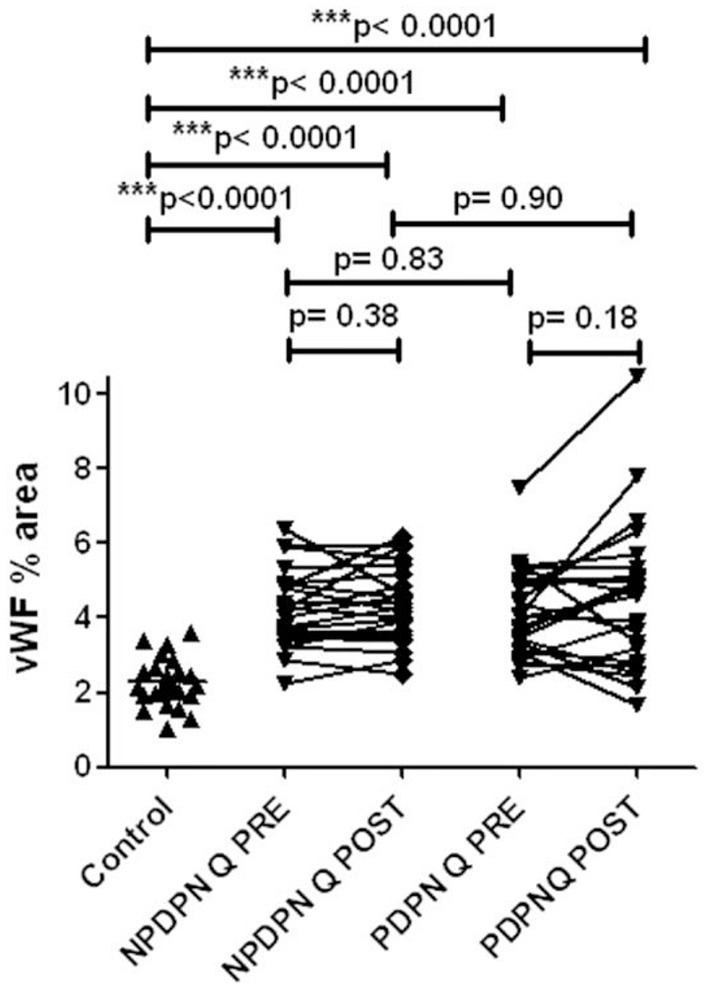
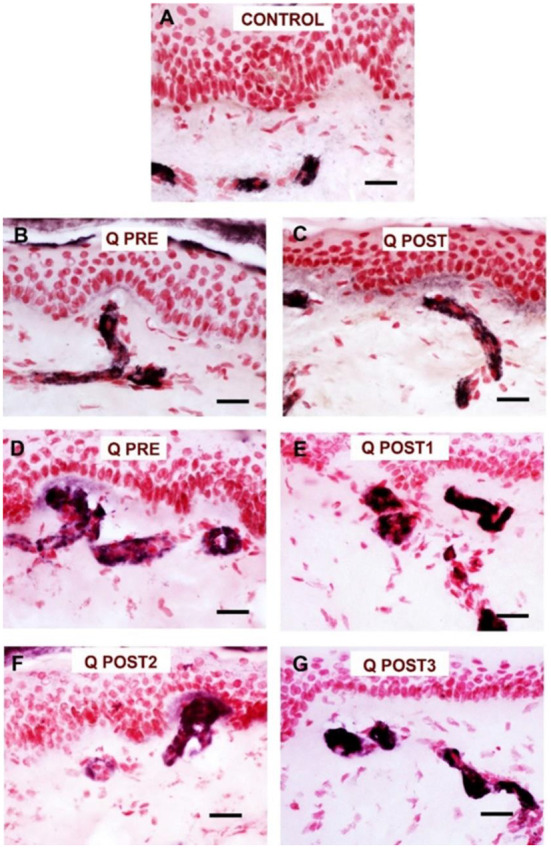
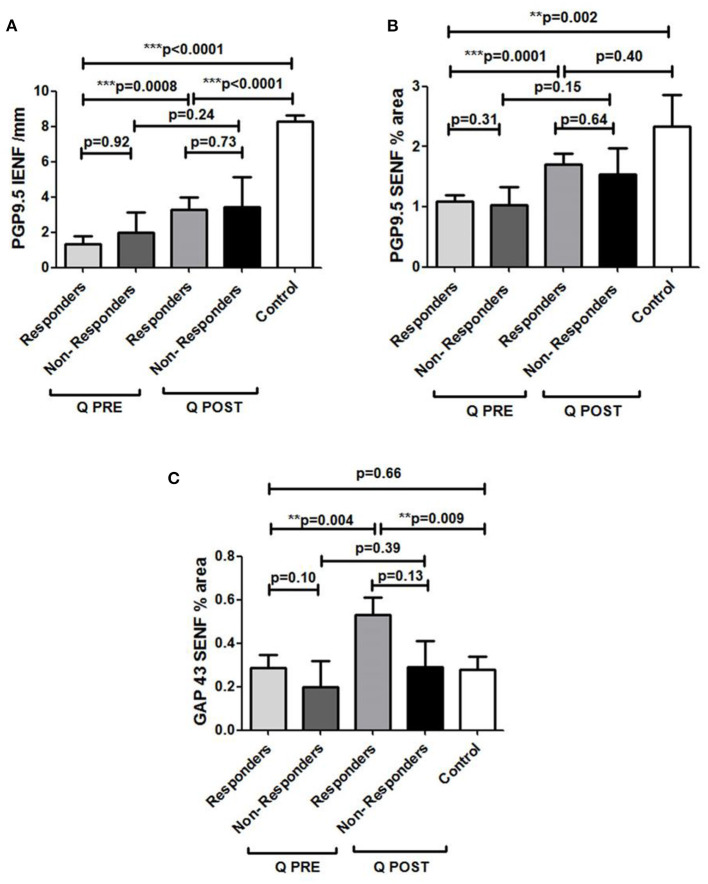
Results: At 3 months after baseline, PDPN Q+SOC group had reduction in NPRS score (p = 0.0001), but not PDPN SOC group. Short-Form McGill Pain Questionnaire (SF-MPQ) showed significant reductions in scores for overall and other pain descriptors only in the PDPN Q+SOC group. Warm perception thresholds were significantly improved only in the PDPN Q+SOC group (p = 0.02), and correlated with reduction in SF-MPQ overall pain score (p = 0.04). NPDPN Q+SOC group did not report pain during the entire study. Density of intra-epidermal nerve fibers (IENF) with PGP9.5 was increased at 3 months in PDPN Q+SOC (p = 0.0002) and NPDPN Q+SOC (p = 0.002) groups, but not in the PDPN SOC group. Increased sub-epidermal nerve fibers (SENF) were observed with GAP43 (marker of regenerating nerve fibers) only in PDPN Q+SOC (p = 0.003) and NPDPN Q+SOC (p = 0.0005) groups. Pain relief in the PDPN Q+SOC group was correlated with the increased PGP9.5 IENF (p = 0.0008) and GAP43 (p = 0.004), whereas those with lack of pain relief showed no such increase; in some subjects pain relief and increased nerve fibers persisted over months. PGP9.5 IENF increase correlated with axon-reflex vasodilatation in a NPDPN Q+SOC subset (p = 0.006).
Conclusions: Capsaicin 8% patch can provide pain relief via nerve regeneration and restoration of function in DPN (disease modification). It may thereby potentially prevent diabetic foot complications, including ulcers.
Keywords: capsaicin; clinical trial; diabetic neuropathy; pain; skin biopsy.
Copyright © 2022 Anand, Privitera, Donatien, Fadavi, Tesfaye, Bravis and Misra.
Conflict of interest statement
This study received supplementary funding from Grünenthal GmbH. The funder had the following involvement with the study: interpretation of data. PA has received symposia speaker fees and advisory board honoraria from Grunenthal, but no personal remuneration for conducting this study. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Gylfadottir SS, Christensen DH, Nicolaisen SK, Andersen H, Callaghan BC, Itani M, et al. . Diabetic polyneuropathy and pain, prevalence, and patient characteristics: a cross-sectional questionnaire study of 5,514 patients with recently diagnosed type 2 diabetes. Pain. (2020) 161:574–83. 10.1097/j.pain.0000000000001744 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources