

Cervical Spondylosis as a Hidden Contributing Factor to Fibromyalgia: A Case Report
- PMID: 36388239
- PMCID: PMC9653028
- DOI: 10.2147/IMCRJ.S382872
Cervical Spondylosis as a Hidden Contributing Factor to Fibromyalgia: A Case Report
Abstract
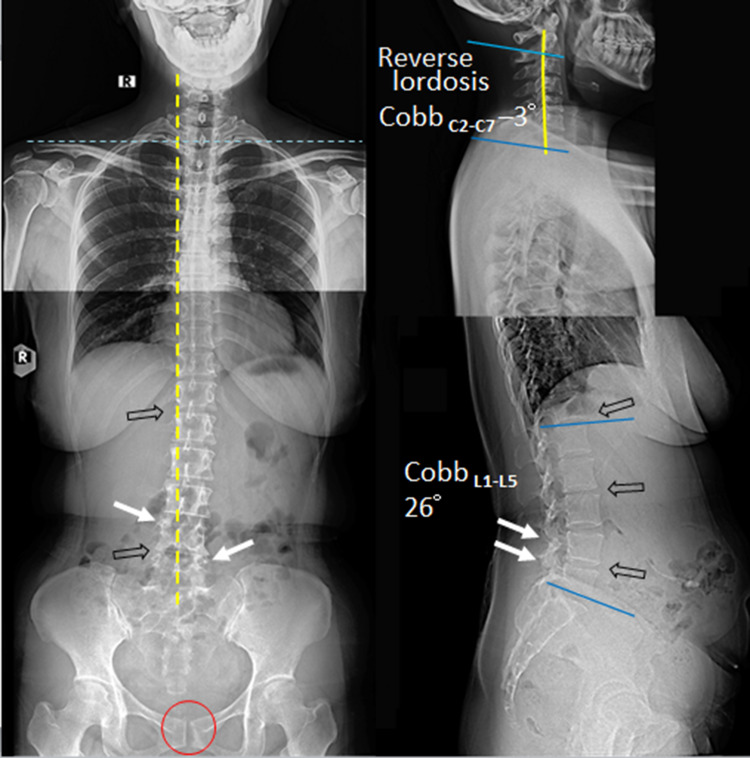
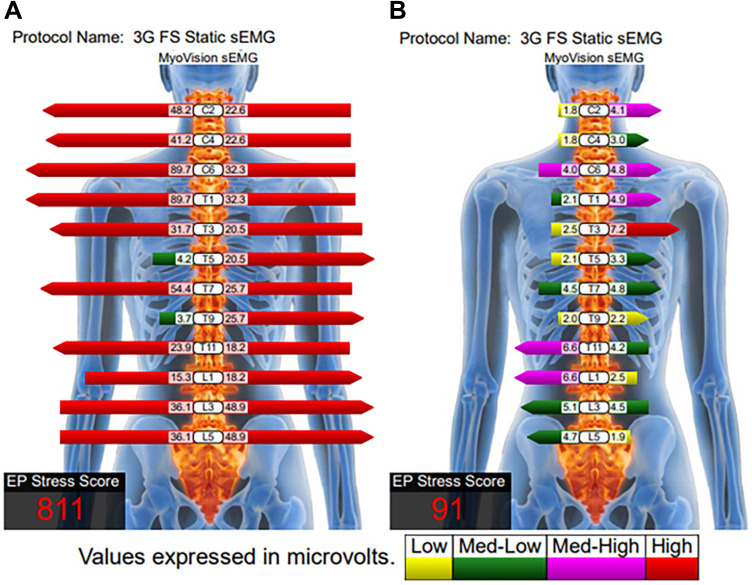
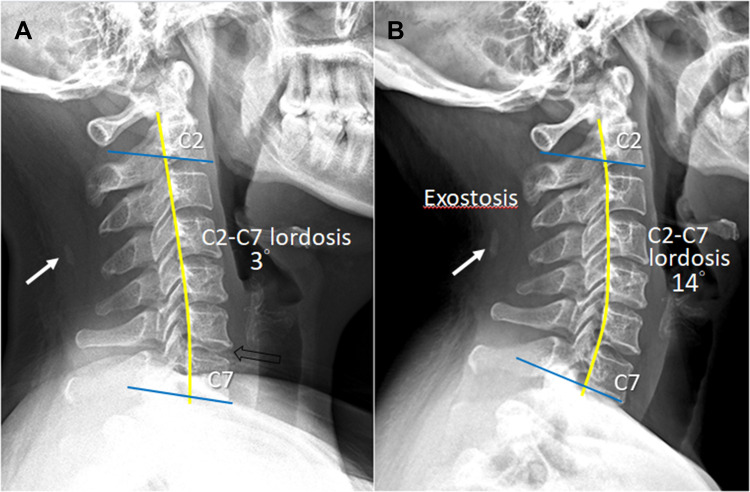
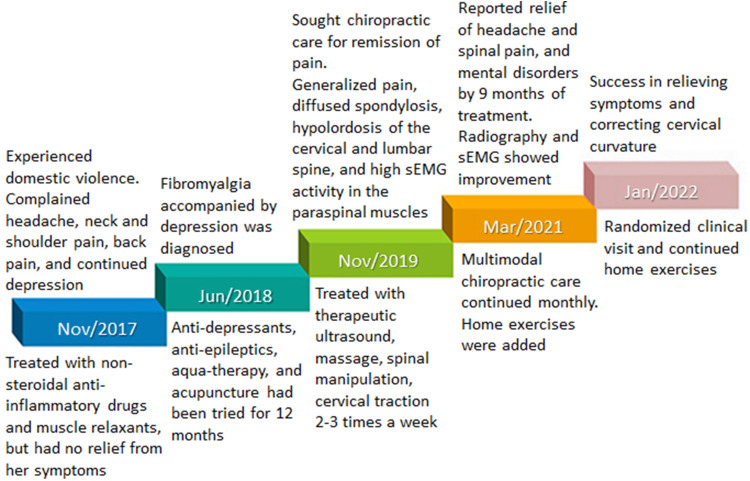
The present case study describes the long-term symptomatic remission in a patient with fibromyalgia (FM) after multimodal spinal manipulation. A 44-year-old woman presented with a chronic headache, severe neck pain, shoulder pain, and back pain lasting for 2 years after experiencing domestic violence. She had sleep disorders, fatigue, and depressive mood. Her primary care physician diagnosed her with FM and comorbid depression. Despite treatment with non-steroidal anti-inflammatory drugs, muscle relaxants, anti-depressants, anti-epileptics, acupuncture, and aqua-therapy, she experienced no appreciable relief from her symptoms. The patient then sought a chiropractic evaluation and potential treatment for her symptoms. At presentation, widespread tenderness was palpable over the neck, shoulder, back, anterior chest, abdominal wall, and buttock. Radiographs showed loss of cervical lordosis, widespread degenerative spondylosis, and osteitis pubis. Surface electromyography (sEMG) revealed neck and thoracic paraspinal muscular spasms. The patient was diagnosed with FM based on the American College of Rheumatology diagnostic criteria and the associated comorbidities. Multimodal chiropractic approaches, which consisted of spinal manipulation, massage, and intermittent motorized cervical traction, were used twice weekly to relieve soft-tissues and intervertebral joints and stretch core musculatures. The patient's physical and mental complaints were mostly resolved near the end of 9 months of treatment. Her symptom alleviation was associated with corresponding change in normalized sEMG signal and cervical spine realignment at the 16th- and 26th-month follow-ups. Widespread pain in FM can lead to confused thinking and a lack of awareness of cervical spondylosis. In this example, it is assumed that the noxious cervical inputs triggered an ongoing FM process. Chiropractic treatment blocked noxious inputs coming from pain sources, corrected pain thresholds, and lowered excitability, thereby eradicating FM symptoms.
Keywords: chiropractic; degenerative spondylosis; electromyography; fibromyalgia; neck pain.
© 2022 Chu and Lee.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Harte SE, Harris RE, Clauw DJ. The neurobiology of central sensitization. J Appl Behav Res. 2018;23(2):e12137. doi: 10.1111/jabr.12137 - DOI
Publication types
LinkOut - more resources
Full Text Sources
