

Evaluation of a clinical decision support system for detection of patients at risk after kidney transplantation
- PMID: 36388342
- PMCID: PMC9641169
- DOI: 10.3389/fpubh.2022.979448
Evaluation of a clinical decision support system for detection of patients at risk after kidney transplantation
Abstract
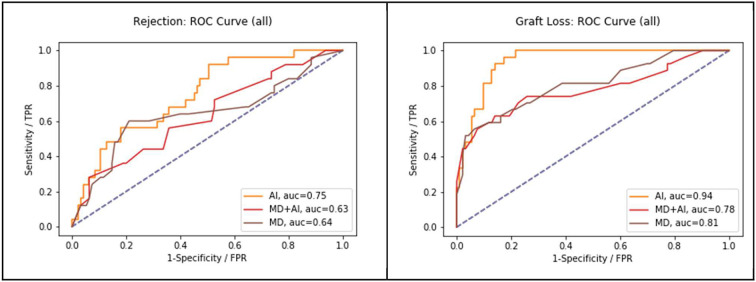
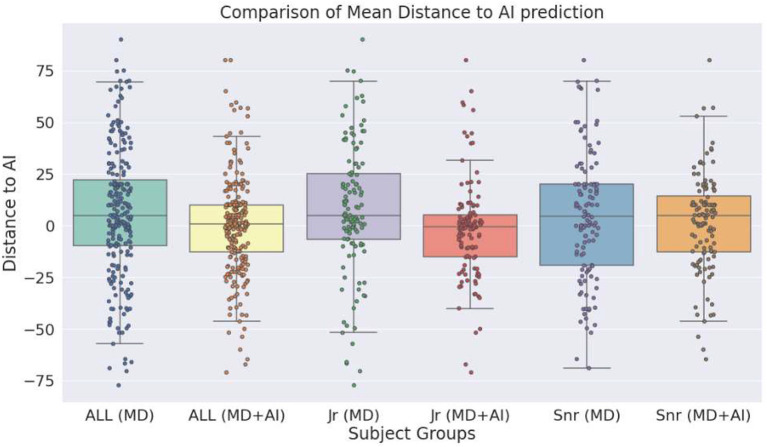
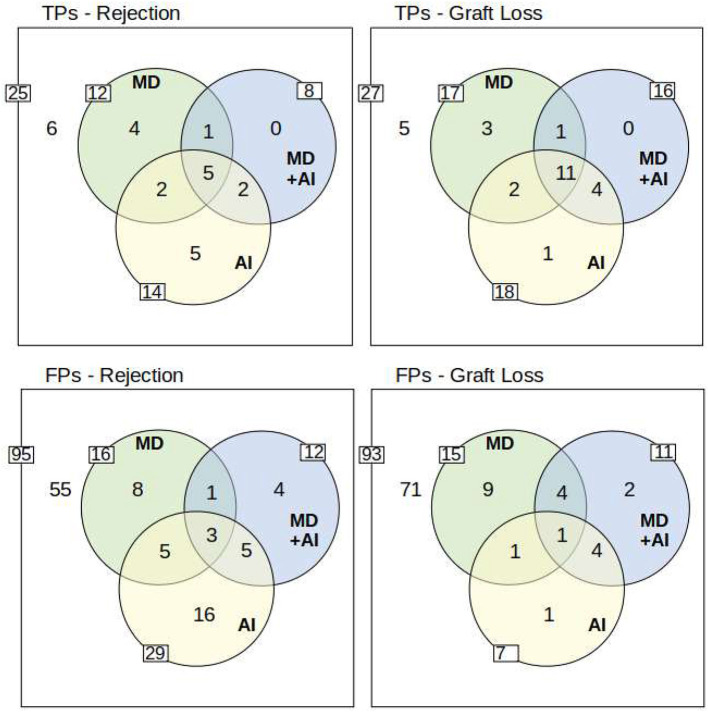
Patient care after kidney transplantation requires integration of complex information to make informed decisions on risk constellations. Many machine learning models have been developed for detecting patient outcomes in the past years. However, performance metrics alone do not determine practical utility. We present a newly developed clinical decision support system (CDSS) for detection of patients at risk for rejection and death-censored graft failure. The CDSS is based on clinical routine data including 1,516 kidney transplant recipients and more than 100,000 data points. In a reader study we compare the performance of physicians at a nephrology department with and without the CDSS. Internal validation shows AUC-ROC scores of 0.83 for rejection, and 0.95 for graft failure. The reader study shows that predictions by physicians converge toward the CDSS. However, performance does not improve (AUC-ROC; 0.6413 vs. 0.6314 for rejection; 0.8072 vs. 0.7778 for graft failure). Finally, the study shows that the CDSS detects partially different patients at risk compared to physicians. This indicates that the combination of both, medical professionals and a CDSS might help detect more patients at risk for graft failure. However, the question of how to integrate such a system efficiently into clinical practice remains open.
Keywords: decision support (DS); graft failure; kidney transplantation; machine learning; rejection.
Copyright © 2022 Roller, Mayrdorfer, Duettmann, Naik, Schmidt, Halleck, Hummel, Burchardt, Möller, Dabrock, Osmanodja and Budde.
Conflict of interest statement
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous