

Molecular Biomarkers for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis
- PMID: 36388432
- PMCID: PMC9664479
- DOI: 10.1016/j.euros.2022.10.017
Molecular Biomarkers for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis
Abstract
Context: Prostate cancer (PCa) is the second most common type of cancer in men. Individualized risk stratification is crucial to adjust decision-making. A variety of molecular biomarkers have been developed in order to identify patients at risk of clinically significant PCa (csPCa) defined by the most common PCa risk stratification systems.
Objective: The present study aims to examine the effectiveness (diagnostic accuracy) of blood or urine-based PCa biomarkers to identify patients at high risk of csPCa.
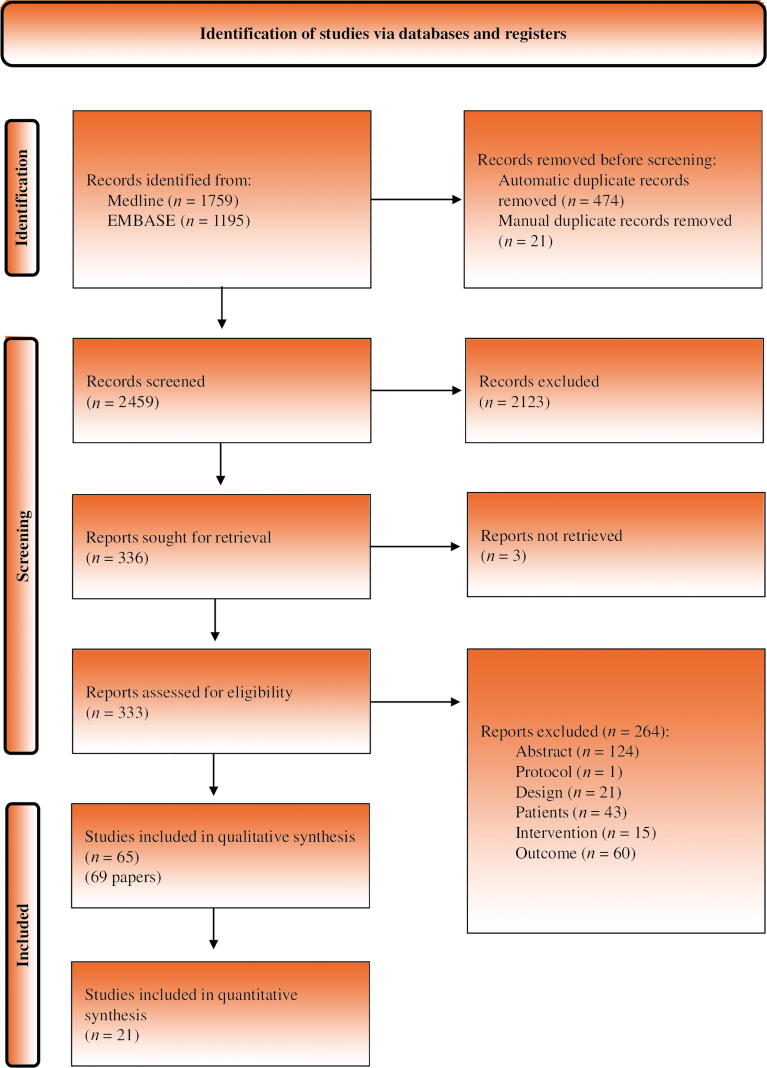
Evidence acquisition: A systematic review of the literature was conducted. Medline and EMBASE were searched from inception to March 2021. Randomized or nonrandomized clinical trials, and cohort and case-control studies were eligible for inclusion. Risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool. Pooled estimates of sensitivity, specificity, and area under the curve were obtained.
Evidence synthesis: Sixty-five studies (N = 34 287) were included. Not all studies included prostate-specific antigen-selected patients. The pooled data showed that the Prostate Health Index (PHI), with any cutoff point between 15 and 30, had sensitivity of 0.95-1.00 and specificity of 0.14-0.33 for csPCa detection. The pooled estimates for SelectMDx test sensitivity and specificity were 0.84 and 0.49, respectively.
Conclusions: The PHI test has a high diagnostic accuracy rate for csPCa detection, and its incorporation in the diagnostic process could reduce unnecessary biopsies. However, there is a lack of evidence on patient-important outcomes and thus more research is needed.
Patient summary: It has been possible to verify that the application of biomarkers could help detect prostate cancer (PCa) patients with a higher risk of poorer evolution. The Prostate Health Index shows an ability to identify 95-100 for every 100 patients suffering from clinically significant PCa who take the test, preventing unnecessary biopsies in 14-33% of men without PCa or insignificant PCa.
Keywords: Clinically significant cancer; Meta-analysis; Molecular markers; Prostatic neoplasms; Systematic review.
© 2022 The Authors.
Figures











References
-
- Sung H., Ferlay J., Siegel R.L., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71:209–249. - PubMed
-
- Torre L.A., Siegel R.L., Ward E.M., Jemal A. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Biomarkers Prev. 2016;25:16–27. - PubMed
-
- Ferlay J., Ervik M., Lam F., et al. International Agency for Research on Cancer; Lyon, France: 2020. Global cancer observatory: cancer today; p. 419.
-
- National Cancer Institute . National Institutes of Health; Bethesda, MD: 2019. SEER cancer stat facts.https://seer.cancer.gov/statfacts/html/mulmy.html
Publication types
LinkOut - more resources
Full Text Sources
