

Uterine transarterial embolization as nonsurgical management for uterine rupture following vaginal delivery: A report of two cases
- PMID: 36388613
- PMCID: PMC9661432
- DOI: 10.1016/j.radcr.2022.10.031
Uterine transarterial embolization as nonsurgical management for uterine rupture following vaginal delivery: A report of two cases
Abstract
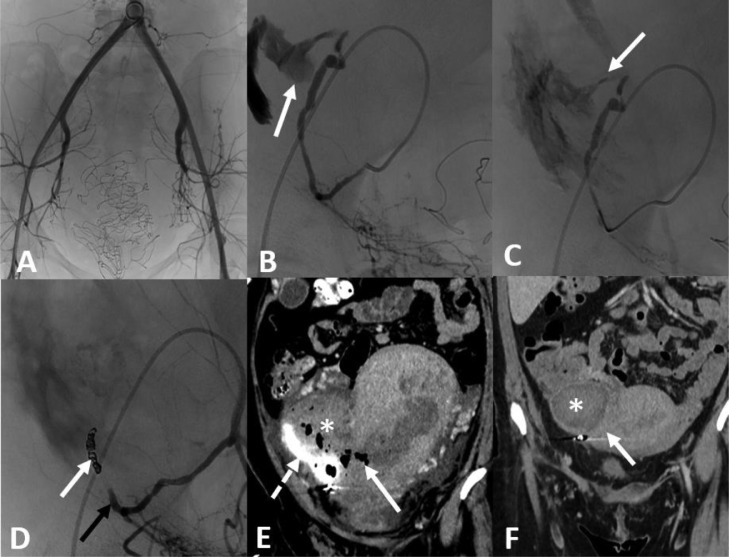
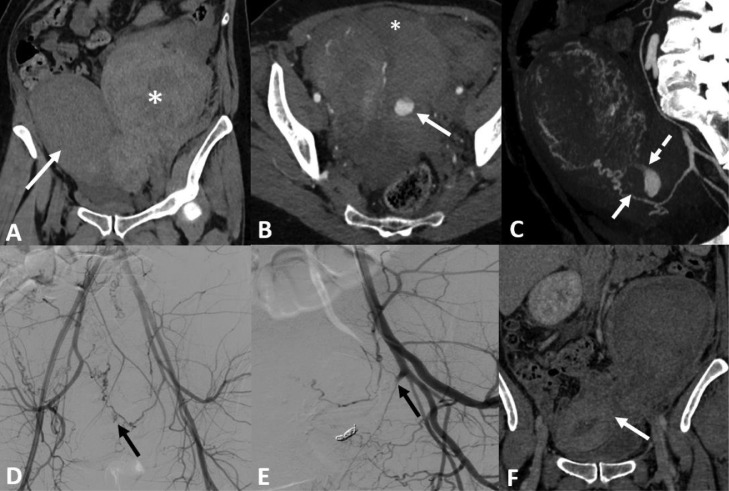
Uterine rupture (UR) is an unexpected, rare, and serious obstetrical condition, occurring in less than 0.1% of pregnancies. Complete UR is defined as a direct communication between the uterine cavity and the peritoneum due to a complete rupture of the myometrium. Here, we present 2 cases of non-surgical management of UR following vaginal delivery, which were both treated by uterine transarterial embolization (UAE). A 26-year-old woman (G0P0) was referred to the emergency ward at 35 weeks of amenorrhea to treat the rupture of membranes, in the context of twin pregnancy. A vaginal delivery was performed and blood loss exceeded 2 liters. Gelatin sponge was injected in an attempt to occlude the right uterine artery. The injection was unsuccessful. After the medical team's discussion, it was decided to definitively occlude the right uterine artery. A 37-year-old woman (G3P3) was referred for a vaginal delivery for a medical termination at 38 weeks of amenorrhea. The ultrasound revealed a left latero-uterine pelvic hematoma, suggestive of UR. Four fibered coils were used to definitively occlude the left uterine artery. Computed tomography scan showed a progressive resorption of hematoma and satisfactory enhancement of the uterine wall in the 2 cases. Transarterial embolization may allow for bleeding to stop without resorting to exploratory laparotomy, with ad-integrum restitution of the uterine wall, and thus prevent a potential hysterectomy. The findings in these 2 cases suggest that UAE should be considered if pregnant women develop UR after delivery.
Keywords: Coils; Embolization; Hemorrhage; Uterine rupture.
© 2022 The Authors.
Figures
References
-
- Donati S, Fano V, Maraschini A, Regional Obstetric Surveillance System Working Group Uterine rupture: results from a prospective population-based study in Italy. Eur J Obstet Gynecol Reprod Biol. 2021;264:70–75. - PubMed
-
- Hofmeyr GJ, Say L, Gülmezoglu AM. WHO systematic review of maternal mortality and morbidity: the prevalence of uterine rupture. BJOG. 2005;112:1221–1228. - PubMed
-
- Tanos V, Toney ZA. Uterine scar rupture—prediction, prevention, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol. 2019;59:115–131. - PubMed
-
- Vandenberghe G, Bloemenkamp K, Berlage S, Colmorn L, Deneux-Tharaux C, Gissler M, et al. The International Network of Obstetric Survey Systems study of uterine rupture: a descriptive multi-country population-based study. BJOG. 2019;126:370–381. - PubMed
-
- Aboughalia H, Basavalingu D, Revzin MV, Sienas LE, Katz DS, Moshiri M. Imaging evaluation of uterine perforation and rupture. Abdom Radiol. 2021;46:4946–4966. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
