

A randomized controlled trial of positive end-expiratory pressure on pulmonary oxygenation and biventricular function in esophageal cancer patients receiving one-lung ventilation under a lower FiO2
- PMID: 36388664
- PMCID: PMC9660073
- DOI: 10.21037/jgo-22-522
A randomized controlled trial of positive end-expiratory pressure on pulmonary oxygenation and biventricular function in esophageal cancer patients receiving one-lung ventilation under a lower FiO2
Abstract
Background: Arterial oxygenation is often impaired during one-lung ventilation (OLV), due to both pulmonary shunt and atelectasis. Lower fraction of inspiration O2 (FiO2) may reduce inflammation and complications, but may increase the risk of hypoxemia. The aim of this randomized controlled parallel trial was to analyze whether higher positive end-expiratory pressure (PEEP) could improve oxygenation and maintain lower levels of inflammation during OLV under a lower FiO2.
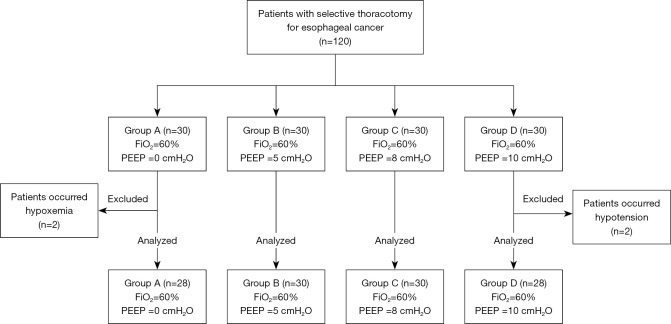
Methods: One hundred and twenty patients with selective thoracotomy for esophageal cancer (EC) were classified randomly into four groups on a ratio of 1:1:1:1 using a computer-generated list, including Group A (FiO2 =0.6, PEEP =0), Group B (FiO2 =0.6, PEEP =5 cmH2O), Group C (FiO2 =1.0, PEEP =8 cmH2O), and Group D (FiO2 =1.0, PEEP =10 cmH2O). The oxygenation and pulmonary shunt were primary outcomes. Haemodynamics, respiratory mechanics, serum IL-6 and IL-10 levels, and complications were taken as secondary outcomes. Follow-up was terminated until discharge.
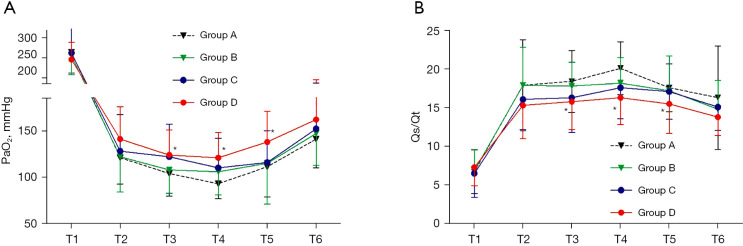
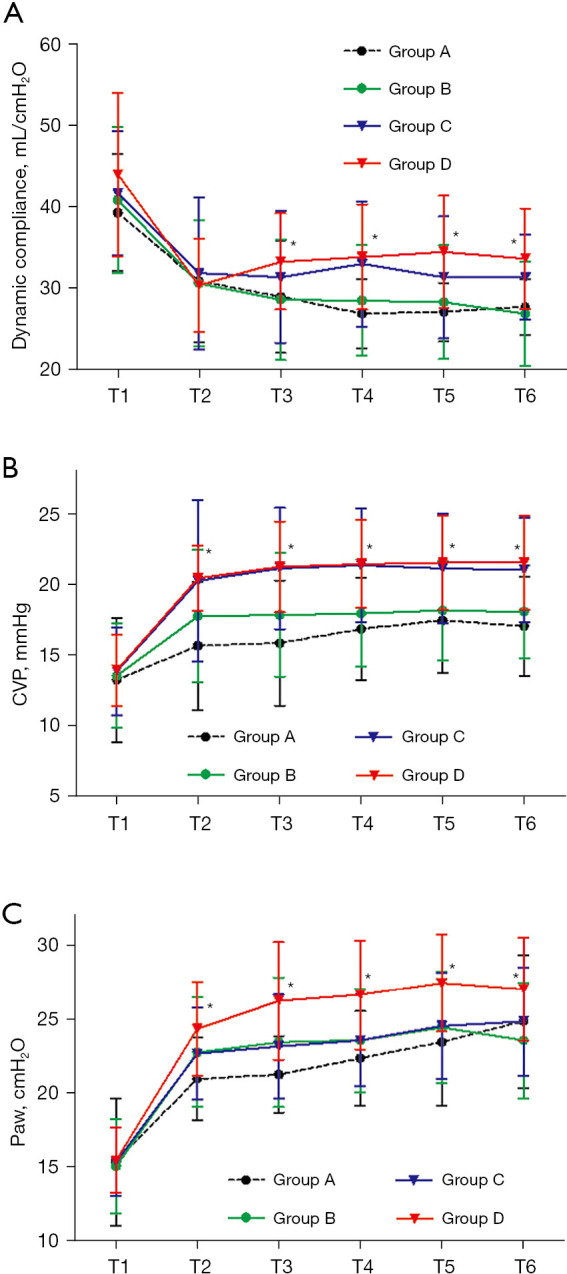
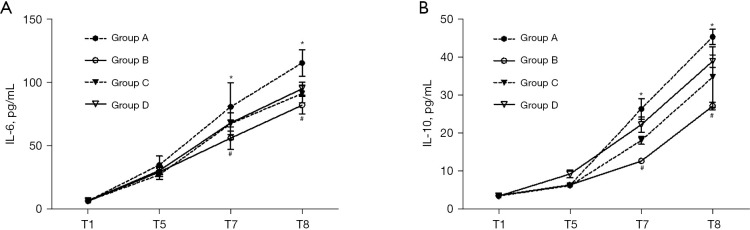
Results: Two patients in Group A and two in Group D were excluded due to hypoxemia and hypotension, respectively. Then the data of 116 patients (Group A =28, Group B =30 Group C =30, and Group D =28) were assessed for final analysis. Compared with Group B, the partial pressure of oxygen (PaO2) and dynamic compliance during OLV in Group D were significantly increased from 15 minutes to 60 minutes, while pulmonary shunt was significantly decreased (P>0.05). Patients in Group D had higher levels of central venous pressure (CVP) and airway pressure (Paw) during OLV and higher levels of IL-6 and IL-10 after OLV compared with Group B (P>0.05). No statistical differences were found in oxygen saturation (SaO2), PvO2 (partial pressure of oxygen in venous blood), partial pressure of end-tidal carbon dioxide (ETCO2), partial pressure of carbon dioxide in artery (PaCO2), heart rate (HR), mean arterial pressure (MAP), and complications among the four groups (P>0.05).
Conclusions: Higher PEEP increased the oxygenation under 60% O2 during OLV. However, the haemodynamics and respiratory mechanics changed, and the levels of inflammation increased. A higher PEEP under 60% O2 during OLV is not recommended.
Trial registration: Chinese Clinical Trial Registry ChiCTR1900024726.
Keywords: Positive end-expiratory pressure (PEEP); low FiO2; one-lung ventilation.
2022 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-522/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Effects of prostaglandin E1 nebulization of ventilated lung under 60%O2 one lung ventilation on patients' oxygenation and oxidative stress: a randomised controlled trial.Respir Res. 2020 May 13;21(1):113. doi: 10.1186/s12931-020-01380-6. Respir Res. 2020. PMID: 32404117 Free PMC article. Clinical Trial.
-
Effects of different positive end-expiratory pressure titrating strategies on oxygenation and respiratory mechanics during one- lung ventilation: a randomized controlled trial.Ann Palliat Med. 2021 Feb;10(2):1133-1144. doi: 10.21037/apm-19-441. Epub 2020 Sep 15. Ann Palliat Med. 2021. PMID: 32954753 Clinical Trial.
-
Effects of positive end-expiratory pressure on regional cerebral oxygen saturation in elderly patients undergoing thoracic surgery during one-lung ventilation: a randomized crossover-controlled trial.BMC Pulm Med. 2024 Mar 6;24(1):120. doi: 10.1186/s12890-024-02931-z. BMC Pulm Med. 2024. PMID: 38448844 Free PMC article. Clinical Trial.
-
Impact of a positive end-expiratory pressure strategy on oxygenation, respiratory compliance, and hemodynamics during laparoscopic surgery in non-obese patients: a systematic review and meta-analysis of randomized controlled trials.BMC Anesthesiol. 2023 Nov 11;23(1):371. doi: 10.1186/s12871-023-02337-0. BMC Anesthesiol. 2023. PMID: 37950169 Free PMC article.
-
Individualised positive end-expiratory pressure in abdominal surgery: a systematic review and meta-analysis.Br J Anaesth. 2022 Nov;129(5):815-825. doi: 10.1016/j.bja.2022.07.009. Epub 2022 Aug 26. Br J Anaesth. 2022. PMID: 36031417
Cited by
-
Effect of target-controlled pressure-controlled ventilation on percutaneous nephrolithotripsy patients under general anesthesia: a retrospective study.Transl Androl Urol. 2023 May 31;12(5):727-735. doi: 10.21037/tau-23-158. Epub 2023 Apr 17. Transl Androl Urol. 2023. PMID: 37305637 Free PMC article.
References
LinkOut - more resources
Full Text Sources