

Contemporary Management of Intracranial Subdural Empyema: An Institutional Experience
- PMID: 36388740
- PMCID: PMC9641731
- DOI: 10.4103/jwas.jwas_127_22
Contemporary Management of Intracranial Subdural Empyema: An Institutional Experience
Abstract
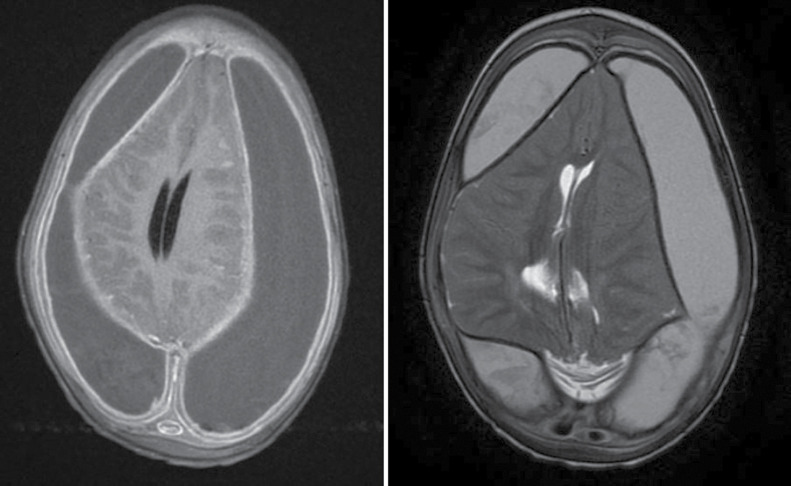
Background: Intracranial subdural empyema (SDE) is a seemingly uncommon life-threatening ailment with varying presentations and outcomes. A variety of risk factors have been associated with predisposition to intracranial SDEs; however, they may be cryptogenic. There is an increased predilection for intracranial SDE in children and teenagers with paranasal sinusitis or middle ear infections. The clinical presentation is non-specific and thus a high index of suspicion is required. Neuroimaging is an invaluable diagnostic tool for early diagnosis and surgical intervention. There have been multiple proponents for either burr hole or craniotomy to treat intracranial SDEs; however, despite surgical intervention, adverse neurologic sequelae and even mortality still occur. Extended antibiotic therapy is mandatory and impacts significantly on patients' outcomes.
Objectives: This study describes the demographics, clinical presentation, and surgical outcomes in patients with intracranial SDEs over the study period.
Design: This is a retrospective single-centre case series.
Setting: This study takes place in a tertiary referral centre, university hospital.
Materials and methods: This was a retrospective review of patients presenting with intracranial SDEs over a 10-year period in a tertiary neurosurgical unit serving south-western Nigeria. Demographic, clinical, and radiologic data were retrieved from patient records.
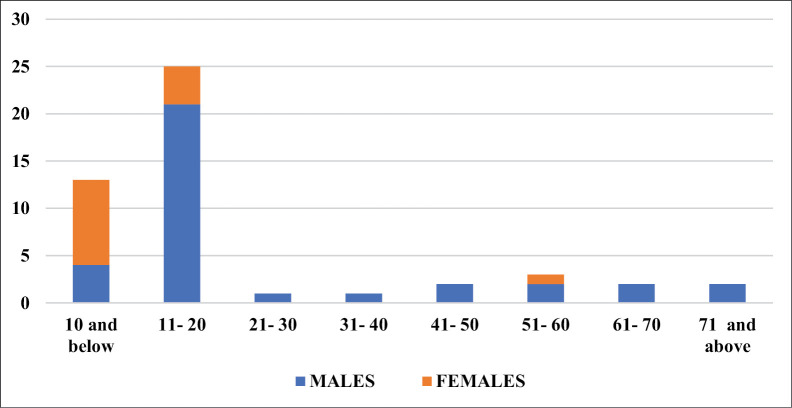
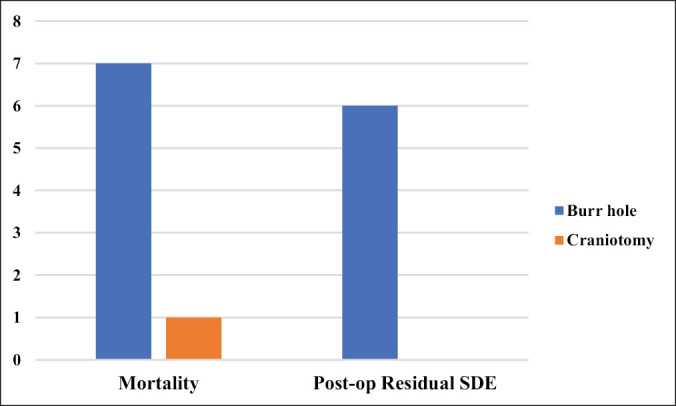
Results: Forty-nine patients presented with intracranial SDEs during the review period. These patients aged between 16 months and 75 years, most of whom were 20 years of age and below. The mean age was 21.37 ± 19.29 years with a median age of 15 years. There were 35 males and 14 females giving a male-to-female ratio of 2.5:1. The most common presentations were headache (73.5%), altered sensorium (55.1%), and seizures (38.8%). Forty patients (81.6%) had evacuation of SDE by burr hole and subdural washout. There was a significant post-op residual SDE in six patients. There were eight (16.3%) mortalities in this series. Forty-seven (95.9%) patients had sterile cultures of the subdural pus collection.
Conclusion: Intracranial SDE affects mostly children and teenagers. Early diagnosis, emergent surgery, extended antibiotic therapy, and concurrent source control employing a multidisciplinary approach are essential in managing this condition. Burr hole and subdural washout help control the disease process, reduce operation time, and may yield outcomes similar to craniotomies, which are more invasive.
Keywords: Antibiotics; Nigeria; burr hole; craniotomy; interhemispheric empyema; sinusitis; subdural empyema (SDE).
Copyright: © 2022 Journal of the West African College of Surgeons.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Agrawal A, Timothy J, Pandit L, Shetty L, Shetty JP. A review of subdural empyema and its management. Infect Dis Clin Pract. 2007;15:149–53.
-
- Yoon J, O’Bryan CM, Redmond M. Intracranial subdural empyema—A mini review. J Infectiol. 2020;3:1–5.
-
- Lefebvre L, Metellus P, Dufour H, Bruder N. Linezolid for treatment of subdural empyema due to Streptococcus: Case reports. Surg Neurol. 2009;71:89–91. discussion 91. - PubMed
-
- De Bonis P, Anile C, Pompucci A, Labonia M, Lucantoni C, Mangiola A. Cranial and spinal subdural empyema. Br J Neurosurg. 2009;23:335–40. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous