

Perspective and practice patterns of mediastinal staging among thoracic surgeons
- PMID: 36389296
- PMCID: PMC9641344
- DOI: 10.21037/jtd-22-183
Perspective and practice patterns of mediastinal staging among thoracic surgeons
Abstract
Background: Accurate mediastinal staging of lung cancer patients is critical for determining appropriate treatment. Mediastinoscopy and endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration are the most commonly utilized techniques. Limited data exist on training and practice trends among thoracic surgeons. We aimed to determine training and practice patterns and find whether there is a paradigm shift in mediastinal staging after the introduction of EBUS into practice among thoracic surgeons in the United States.
Methods: 28-question survey was constructed querying demographic, training, and practice patterns with mediastinoscopy and EBUS and was sent to practicing thoracic surgeons in the United States. Descriptive statistics were used to summarize quantitative data.
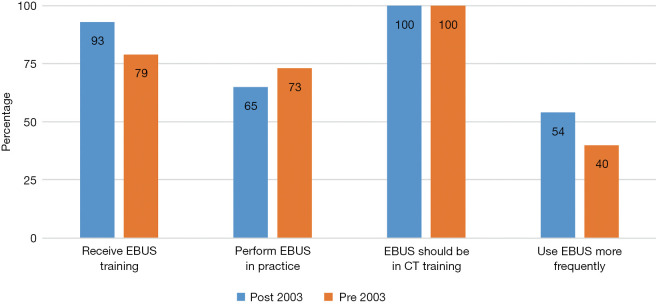
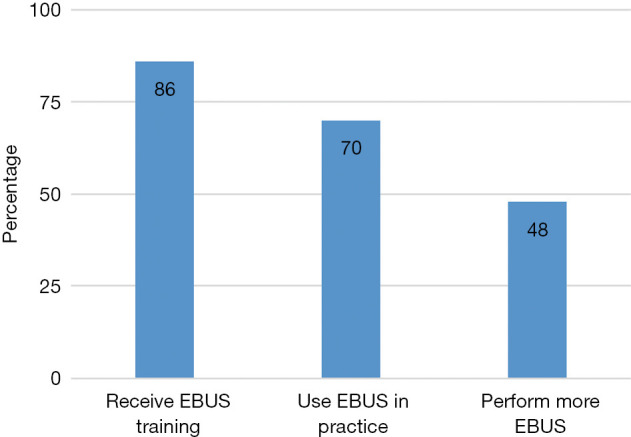
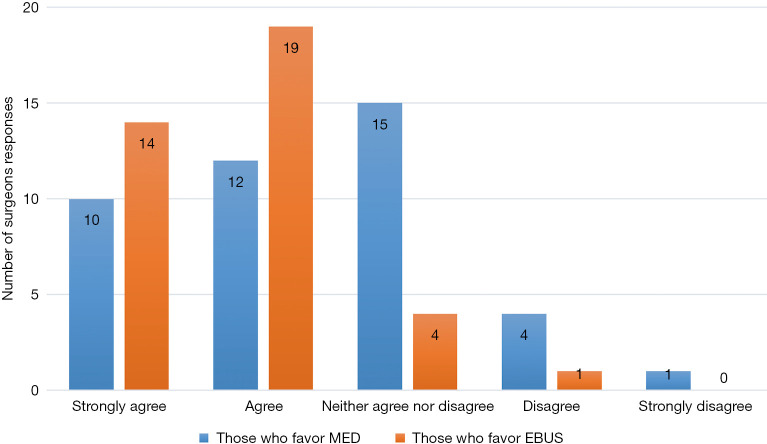
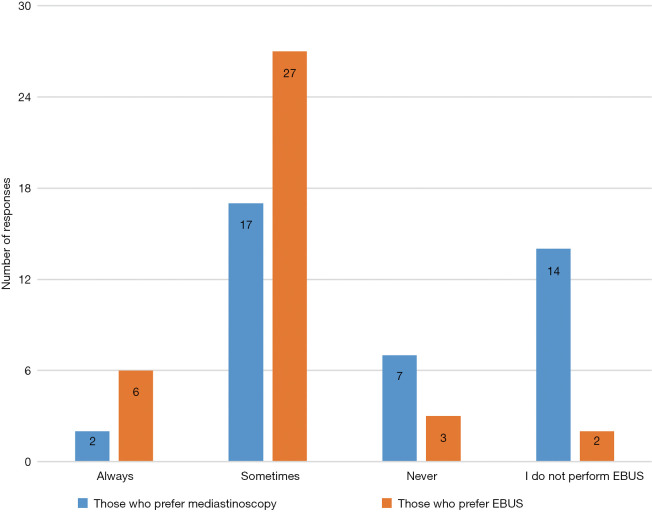
Results: Ninety-eight responded with a 93% completion rate. Eighty-seven percent of respondents received training in EBUS and 70% perform EBUS routinely. All respondents believe EBUS should be incorporated into thoracic surgery training curriculums. Majority of those who prefer EBUS feel EBUS is safer than mediastinoscopy, allows access to lymph nodes stations or lesions inaccessible by mediastinoscopy and prefer EBUS to avoid re-do mediastinoscopy and in irradiated mediastinum. Majority of those who prefer mediastinoscopy reported they perform more accurate staging compared to EBUS, that mediastinoscopy is more accurate in diagnosing lymphoma or sarcoidosis and that frozen section can be done at the same interval as resection. Among surgeons who prefer EBUS, 94% biopsy 3 or more lymph node stations, 86% routinely biopsy hilar (N1) nodes while 8% never biopsy N1 nodes. Of surgeons who prefer mediastinoscopy. Ninety-seven percent biopsy 3 or more lymph node stations, only 27% routinely biopsy N1 nodes and 70% never biopsy N1 nodes.
Conclusions: EBUS is used frequently by thoracic surgeons in their practice for mediastinal staging. Methods of obtaining proficiency in EBUS widely varied among surgeons. In addition to mediastinoscopy, dedicated EBUS training should be incorporated into thoracic surgery training curriculums.
Keywords: Endobronchial ultrasound (EBUS); endoscopic training; mediastinal staging; mediastinoscopy.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-183/coif). The authors have no conflicts of interest to declare.
Figures

Comment in
-
Endobronchial ultrasound transbronchial needle aspiration among thoracic surgeons: to dare is to do.J Thorac Dis. 2022 Dec;14(12):4582-4585. doi: 10.21037/jtd-22-1333. J Thorac Dis. 2022. PMID: 36647479 Free PMC article. No abstract available.
-
Mediastinal staging by thoracic surgeons: are we close to a paradigm shift?J Thorac Dis. 2023 Jan 31;15(1):10-13. doi: 10.21037/jtd-22-1420. Epub 2023 Jan 6. J Thorac Dis. 2023. PMID: 36794129 Free PMC article. No abstract available.
References
-
- National Cancer Institute. SEER Cancer Stat Facts: Lung and Bronchus Cancer [Internet]. 2021 [cited 2021 Dec 27]. Available online: https://seer.cancer.gov/statfacts/html/lungb.html
-
- Huertgen M, Tripsky J, Hartert M. Video-Assisted Mediastinoscopic Lymphadenectomy (VAMLA): Recipe and Cooking Secrets (a Tutorial). Oper Tech Thorac Cardiovasc Surg 2020;25:140-70. 10.1053/j.optechstcvs.2020.05.005 - DOI
-
- Figueiredo VR, Cardoso PFG, Jacomelli M, et al. EBUS-TBNA versus surgical mediastinoscopy for mediastinal lymph node staging in potentially operable non-small cell lung cancer: a systematic review and meta-analysis. J Bras Pneumol 2020;46:e20190221. Erratum in: J Bras Pneumol 2021;47:e20190221errata. 10.36416/1806-3756/e20190221 - DOI - PubMed
LinkOut - more resources
Full Text Sources