

Case report: Focal segmental glomerulosclerosis in a pediatric atypical progeroid syndrome
- PMID: 36389384
- PMCID: PMC9660256
- DOI: 10.3389/fped.2022.1032653
Case report: Focal segmental glomerulosclerosis in a pediatric atypical progeroid syndrome
Abstract
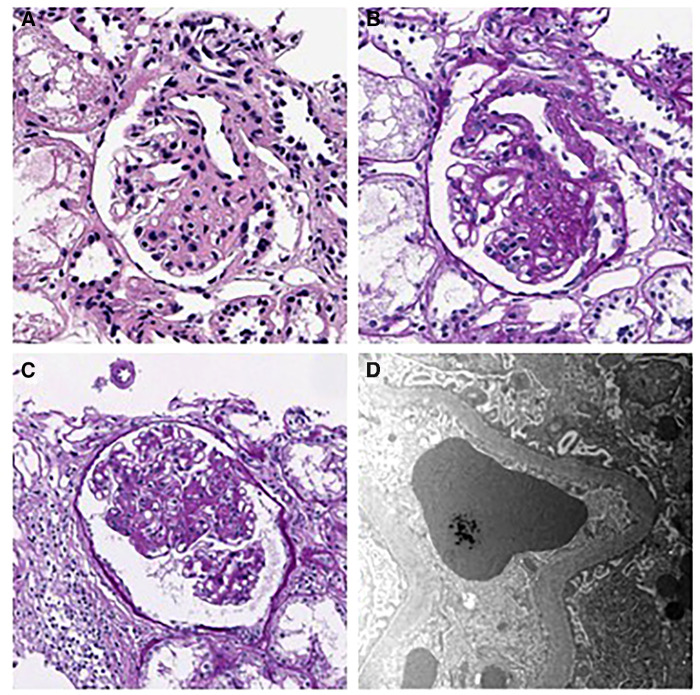
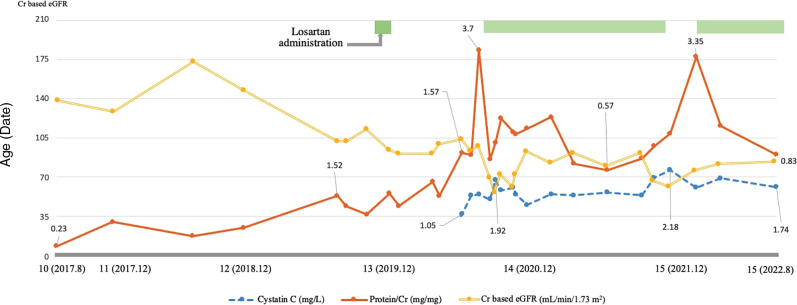
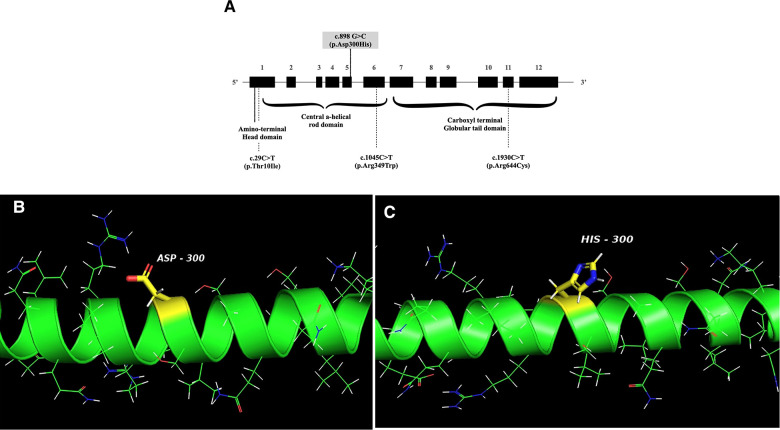
Atypical progeroid syndrome (APS) is a rare type of progeroid syndrome mainly caused by heterozygous missense mutations in the LMNA (MIM 150330) gene. APS has heterogeneous clinical manifestations, and its kidney manifestations, particularly in children, are rarely documented. Here, we report the first pediatric case of APS with focal segmental glomerulosclerosis (FSGS). A 10-year-old boy with progeroid features was referred to the nephrology clinic because of hyperuricemia. He had dark skin, protruding eyes, and beaked nose and was very thin, suggesting lipodystrophy. He had been treated for recurrent urinary tract infection during infancy, and liver biopsy for persisting hepatitis showed steatohepatitis. He also had hypertrophic cardiomyopathy (HCMP) with mitral and tricuspid valve regurgitation. Genetic studies were performed considering his multisystem symptoms, and he was diagnosed as having APS according to exome sequencing findings (c.898G > C, p.Asp300His of LMNA). During the first visit to the nephrology clinic, he had minimal proteinuria (urine protein/creatinine ratio of 0.23 mg/mg), which worsened during follow-up. In three years, his urine protein/creatinine ratio and N-acetyl-b-D-glucosaminidase/creatinine ratio increased to 1.52 and 18.7, respectively. The kidney biopsy result was consistent with findings of FSGS, peri-hilar type, showing segmental sclerosis of 1 (5%) glomerulus out of 21 glomeruli. An angiotensin receptor blocker was added to manage his proteinuria. This is the first pediatric report of FSGS in an APS patient with confirmed LMNA defect, who manifested progeroid features, lipodystrophy, HCMP with heart valve dysfunction, and steatohepatitis. Our case suggests that screening for proteinuric nephropathy is essential for managing APS patients since childhood.
Keywords: LMNA; TGF - β1; atypical progeroid syndrome; focal segmental glomerular sclerosis (FSGS); lipodystrophy.
© 2022 Jang, Ahn, Ko, Ko, Lim and Kang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Multisystem Progeroid Syndrome With Lipodystrophy, Cardiomyopathy, and Nephropathy Due to an LMNA p.R349W Variant.J Endocr Soc. 2020 Jul 27;4(10):bvaa104. doi: 10.1210/jendso/bvaa104. eCollection 2020 Oct 1. J Endocr Soc. 2020. PMID: 32939435 Free PMC article.
-
A Novel Generalized Lipodystrophy-Associated Progeroid Syndrome Due to Recurrent Heterozygous LMNA p.T10I Mutation.J Clin Endocrinol Metab. 2018 Mar 1;103(3):1005-1014. doi: 10.1210/jc.2017-02078. J Clin Endocrinol Metab. 2018. PMID: 29267953 Free PMC article.
-
Atypical Progeroid Syndrome and Partial Lipodystrophy Due to LMNA Gene p.R349W Mutation.J Endocr Soc. 2020 Aug 1;4(10):bvaa108. doi: 10.1210/jendso/bvaa108. eCollection 2020 Oct 1. J Endocr Soc. 2020. PMID: 32913962 Free PMC article.
-
Update on Recurrent Focal Segmental Glomerulosclerosis in Kidney Transplantation.Nephron. 2020;144 Suppl 1:65-70. doi: 10.1159/000510748. Epub 2020 Dec 1. Nephron. 2020. PMID: 33260184 Review.
-
[Focal segmental glomerulosclerosis after renal transplantation in a child with ANCA-associated glomerulonephritis: case report and literature review].Zhonghua Er Ke Za Zhi. 2016 Dec 2;54(12):936-940. doi: 10.3760/cma.j.issn.0578-1310.2016.12.013. Zhonghua Er Ke Za Zhi. 2016. PMID: 27938596 Review. Chinese.
Cited by
-
Podocytopathies associated with familial partial lipodystrophy due to LMNA variants: report of two cases.Arch Endocrinol Metab. 2024 May 10;68:e230204. doi: 10.20945/2359-4292-2023-0204. Arch Endocrinol Metab. 2024. PMID: 38739524 Free PMC article.
-
Deciphering the Clinical Presentations in LMNA-related Lipodystrophy: Report of 115 Cases and a Systematic Review.J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1204-e1224. doi: 10.1210/clinem/dgad606. J Clin Endocrinol Metab. 2024. PMID: 37843397 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous