

Trends in Incidence and Mortality of Larynx Cancer in the US
- PMID: 36394832
- PMCID: PMC9673027
- DOI: 10.1001/jamaoto.2022.3636
Trends in Incidence and Mortality of Larynx Cancer in the US
Abstract
Importance: Larynx cancer is associated with considerable morbidity for patients and has a high mortality rate. Historical analyses showed that the incidence of larynx cancer was decreasing but the mortality was not similarly improving.
Objective: To assess whether incidence and mortality trends in larynx cancer in the US have improved.
Design, setting, and participants: This cohort study used population-based data from the Surveillance, Epidemiology, and End Results Program database for patients older than 18 years who were diagnosed with laryngeal cancer between January 1, 1986, and December 31, 2018. Data were analyzed from May 1, 2021, to May 31, 2022.
Main outcomes and measures: The main outcomes were incidence and mortality of larynx cancer by sex, subsite, and patterns of surgical treatment.
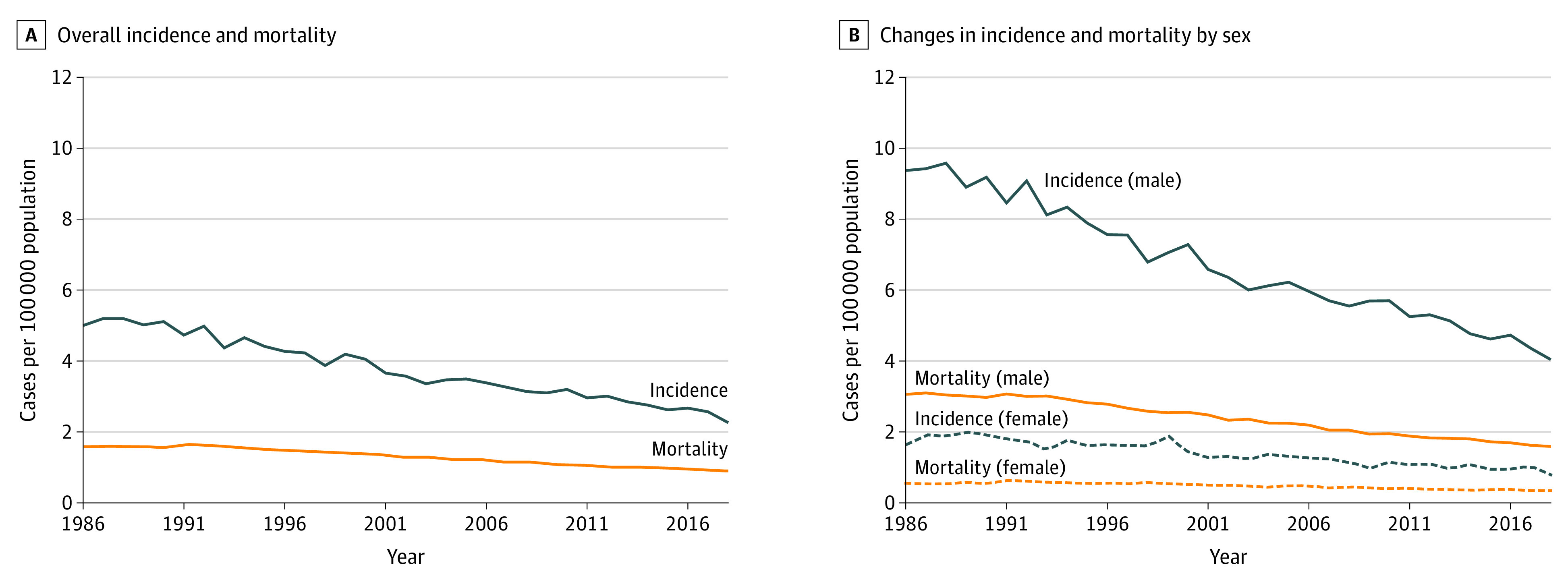
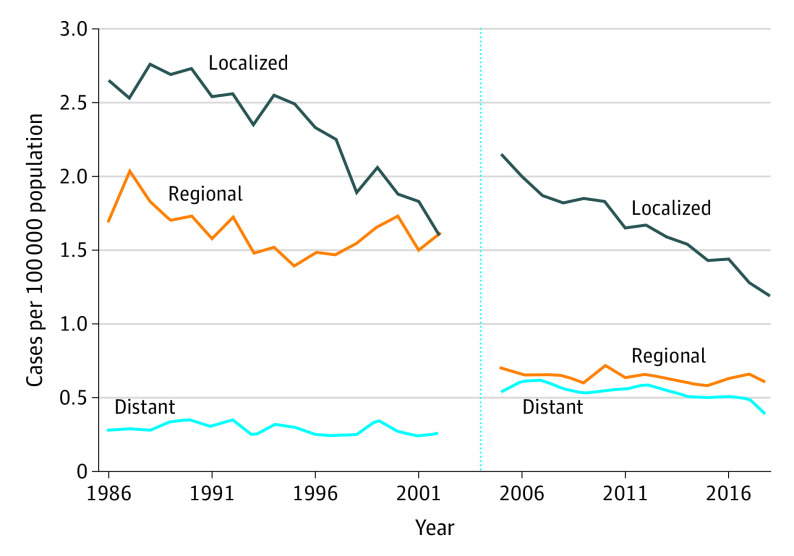
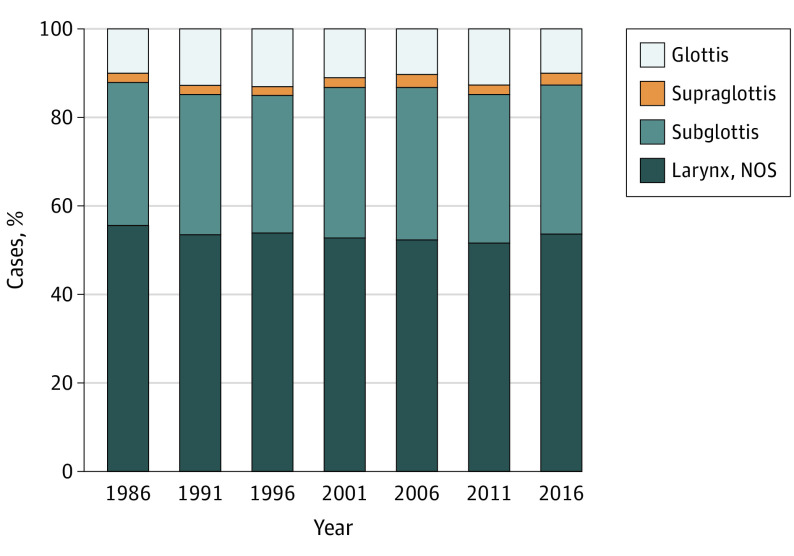
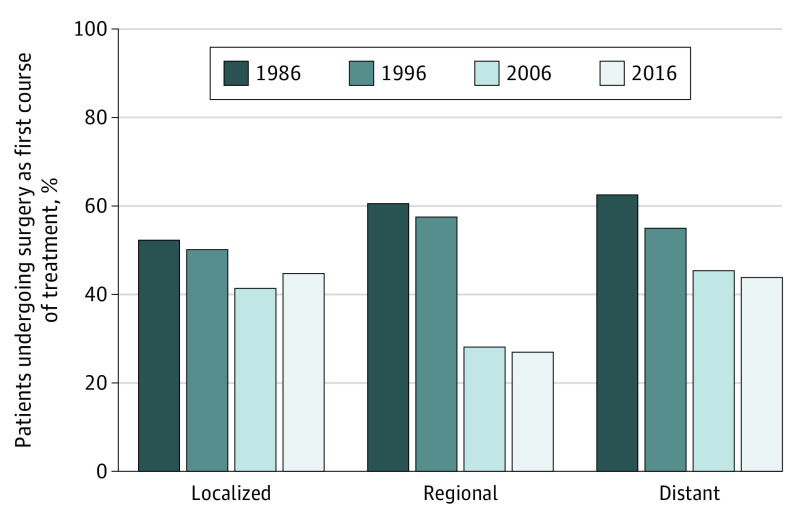
Results: Among 40 850 US patients with larynx cancer diagnosed from 1986 to 2018 (80.4% male), the incidence of larynx cancer decreased 55% from 5.00 per 100 000 people (95% CI, 4.70-5.32 per 100 000 people) to 2.26 per 100 000 people (95% CI, 2.11-2.42 per 100 000 people). During the same period, mortality decreased only 43% from 1.59 per 100 000 people (95% CI, 1.53-1.64 per 100 000 people) to 0.89 per 100 000 people (95% CI, 0.86-0.92 per 100 000 people). This corresponds to a 25% relative increase in case-fatality rate. Examination by stage showed a decrease in the incidence of localized disease at diagnosis of 40% from 2.65 per 100 000 people (95% CI, 2.44-2.89 per 100 000 people) to 1.60 per 100 000 people (95% CI, 1.45-1.76 per 100 000 people) from 1986 to 2002 and of 45% from 2.15 per 100 000 people (95% CI, 1.98-2.34 per 100 000 people) to 1.19 per 100 000 people (95% CI, 1.08-1.31 per 100 000 people) from 2005 to 2018. Distribution of larynx cancer by subsite remained stable, with most cases affecting the glottis. The proportion of patients receiving surgery as their first course of treatment decreased regardless of stage at presentation.
Conclusions and relevance: In this cohort study, between 1986 and 2018, the incidence of larynx cancer decreased in the US, primarily because of the decrease in the incidence of localized disease. Mortality did not decrease similarly, resulting in an increased case-fatality rate overall. Encouraging earlier referrals for cancer concern, focusing resources where larynx cancer rates remain highest, renewing attention to research on new biologic causes of different tumor biologic characteristics, and conducting trials to directly compare treatments may help reverse this trend.
Conflict of interest statement
Figures
References
-
- Wolf GT, Fisher SG, Hong WK, et al. ; Department of Veterans Affairs Laryngeal Cancer Study Group . Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med. 1991;324(24):1685-1690. doi: 10.1056/NEJM199106133242402 - DOI - PubMed
-
- National Cancer Institute . Surveillance, Epidemiology, and End Results Program. Accessed September 15, 2022. http://www.seer.cancer.gov
