

Respiratory and Cardiometabolic Comorbidities and Stages I to III NSCLC Survival: A Pooled Analysis From the International Lung Cancer Consortium
- PMID: 36396063
- PMCID: PMC10463560
- DOI: 10.1016/j.jtho.2022.10.020
Respiratory and Cardiometabolic Comorbidities and Stages I to III NSCLC Survival: A Pooled Analysis From the International Lung Cancer Consortium
Abstract
Introduction: We explored the association of respiratory and cardiometabolic comorbidities with NSCLC overall survival (OS) and lung cancer-specific survival (LCSS), by stage, in a large, multicontinent NSCLC pooled data set.
Methods: On the basis of patients pooled from 11 International Lung Cancer Consortium studies with available respiratory and cardiometabolic comorbidity data, adjusted hazard ratios (aHRs) were estimated using Cox models for OS. LCSS was evaluated using competing risk Grey and Fine models and cumulative incidence functions. Logistic regression (adjusted OR [aOR]) was applied to assess factors associated with surgical resection.
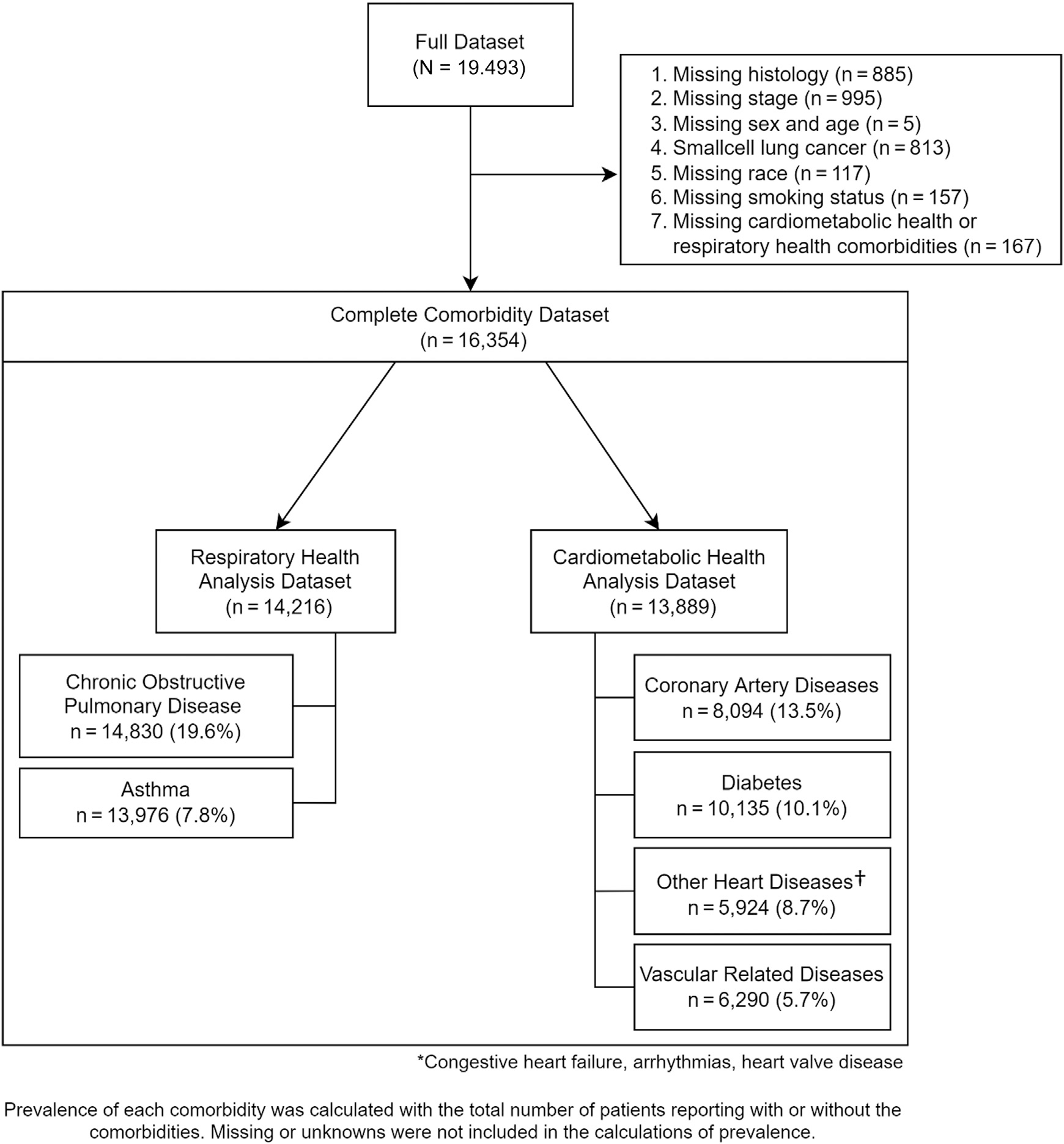
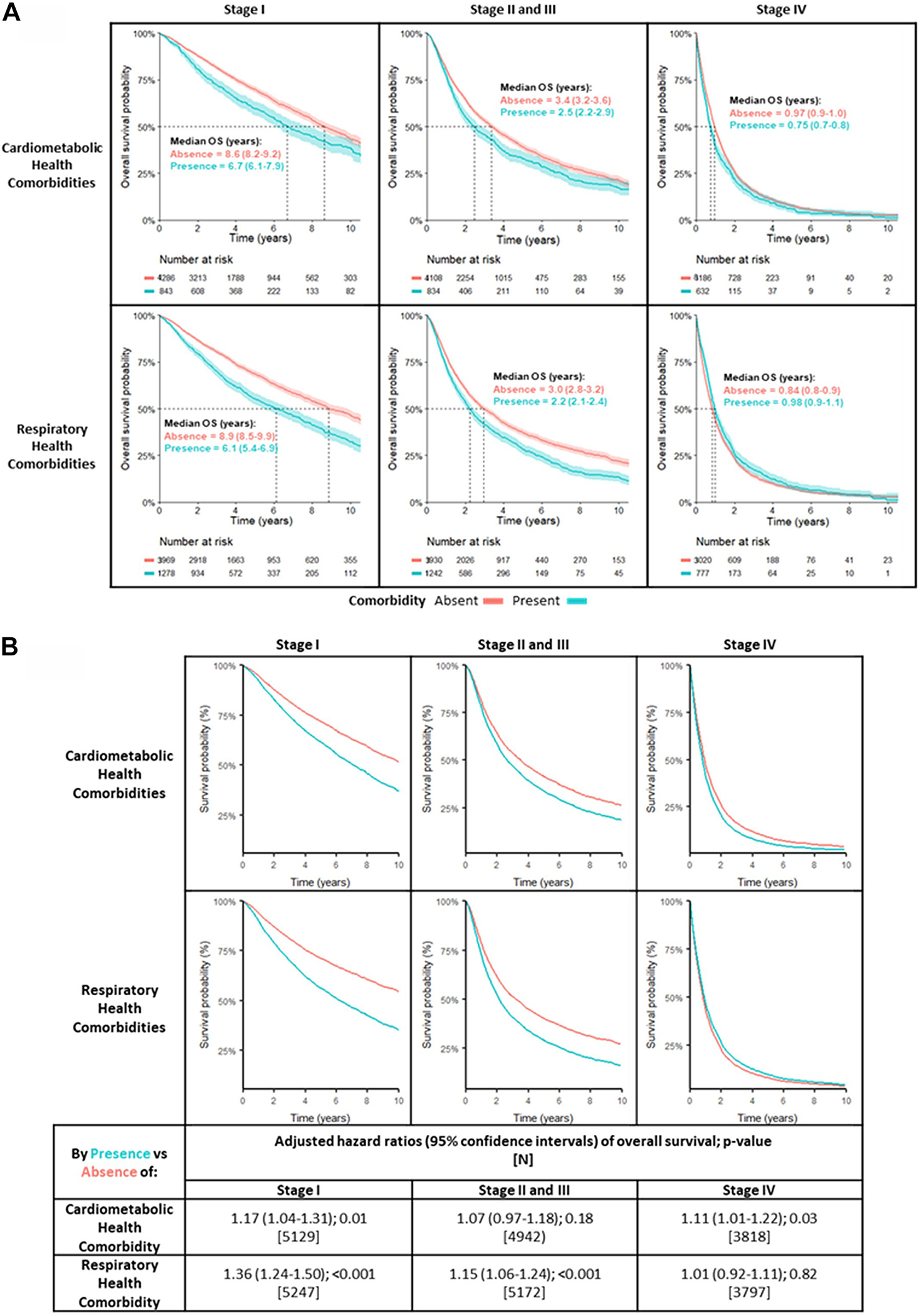
Results: OS analyses used patients with NSCLC with respiratory health or cardiometabolic health data (N = 16,354); a subset (n = 11,614) contributed to LCSS analyses. In stages I to IIIA NSCLC, patients with respiratory comorbidities had worse LCCS (stage IA aHR = 1.51, confidence interval [CI]: 1.17-1.95; stages IB-IIIA aHR = 1.20, CI: 1.06-1.036). In contrast, patients with stages I to IIIA NSCLC with cardiometabolic comorbidities had a higher risk of death from competing (non-NSCLC) causes (stage IA aHR = 1.34, CI: 1.12-1.69). The presence of respiratory comorbidities was inversely associated with having surgical resection (stage IA aOR = 0.54, CI: 0.35-0.83; stages IB-IIIA aOR = 0.57, CI: 0.46-0.70).
Conclusions: The presence of either cardiometabolic or respiratory comorbidities is associated with worse OS in stages I to III NSCLC. Patients with respiratory comorbidities were less likely to undergo surgery and had worse LCSS, whereas patients with cardiometabolic comorbidities had a higher risk of death from competing causes. As more treatment options for stages I to III NSCLC are introduced into the practice, accounting for cardiometabolic and respiratory comorbidities becomes essential in trial interpretation and clinical management.
Keywords: COPD; Comorbidity; Early-stage; NSCLC.
Copyright © 2022. Published by Elsevier Inc.
Conflict of interest statement
Disclosure: Ms. Brown is supported by the Alan B. Brown Chair. Dr. Christiani has received funding through grant U01 CA209414. Prof. Reis and Dr. Leal declare funding from the Public Ministry of Labor Campinas (Research, Prevention, and Education of Occupational Cancer, Brazil). Prof. Chen declares funding from the National Cancer Institute, National Institutes of Health through grants U01-CA063673, UM1-CA167462, and U01-CA167462. Dr. Liu was supported by Alan B. Brown Chair and the Lusi Wong Family Fund, Princess Margaret Cancer Foundation. The remaining authors declare no conflict of interest.
Figures
Comment in
-
An Individualized Approach to Comorbidities in Lung Cancer.J Thorac Oncol. 2023 Mar;18(3):254-256. doi: 10.1016/j.jtho.2022.12.007. J Thorac Oncol. 2023. PMID: 36842806 No abstract available.
-
Comment on "Respiratory and Cardiometabolic Comorbidities and Stages I to III NSCLC Survival: A Pooled Analysis From the International Lung Cancer Consortium".J Thorac Oncol. 2023 Sep;18(9):e95-e96. doi: 10.1016/j.jtho.2023.05.014. J Thorac Oncol. 2023. PMID: 37599054 No abstract available.
-
Re: Response to Letter to the Editor "Respiratory and Cardiometabolic Comorbidities and Stage I-III Non-Small Cell Lung Cancer (NSCLC) Survival: A Pooled Analysis From the International Lung Cancer Consortium".J Thorac Oncol. 2023 Sep;18(9):e96-e97. doi: 10.1016/j.jtho.2023.06.003. J Thorac Oncol. 2023. PMID: 37599055 No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382:41–50. - PubMed
-
- Reck M, Rodríguez-Abreu D, Robinson AG, et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. 2019;37:537–546. - PubMed
-
- Peters S, Camidge DR, Shaw AT, et al. Alectinib versus crizotinib in untreated ALK-positive non–small-cell lung cancer. N Engl J Med. 2017;377:829–838. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
