Effects of intubation timing in patients with COVID-19 throughout the four waves of the pandemic: a matched analysis
- PMID: 36396142
- PMCID: PMC9686319
- DOI: 10.1183/13993003.01426-2022
Effects of intubation timing in patients with COVID-19 throughout the four waves of the pandemic: a matched analysis
Abstract
Background: The primary aim of our study was to investigate the association between intubation timing and hospital mortality in critically ill patients with coronavirus disease 2019 (COVID-19)-associated respiratory failure. We also analysed both the impact of such timing throughout the first four pandemic waves and the influence of prior noninvasive respiratory support on outcomes.
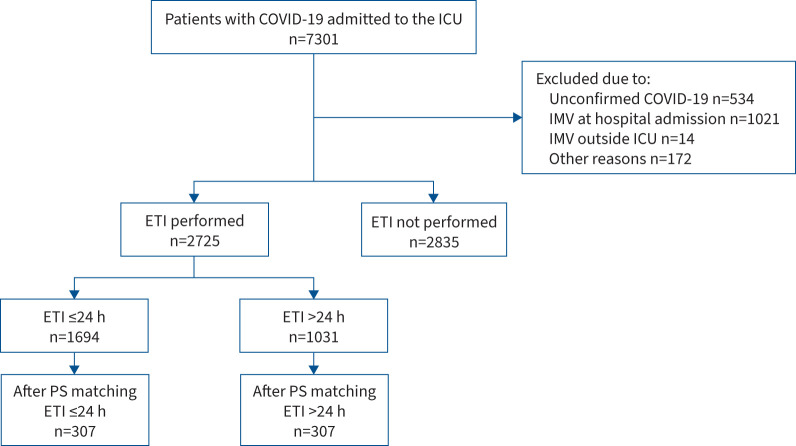
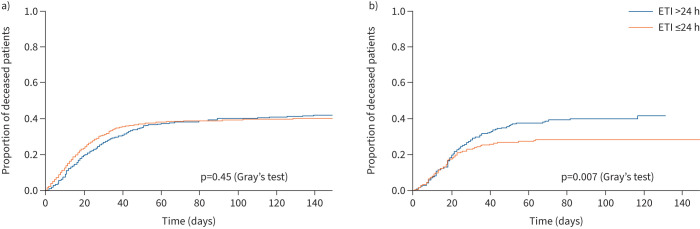
Methods: This is a secondary analysis of a multicentre, observational and prospective cohort study that included all consecutive patients undergoing invasive mechanical ventilation due to COVID-19 from across 58 Spanish intensive care units (ICUs) participating in the CIBERESUCICOVID project. The study period was between 29 February 2020 and 31 August 2021. Early intubation was defined as that occurring within the first 24 h of ICU admission. Propensity score matching was used to achieve a balance across baseline variables between the early intubation cohort and those patients who were intubated after the first 24 h of ICU admission. Differences in outcomes between early and delayed intubation were also assessed. We performed sensitivity analyses to consider a different time-point (48 h from ICU admission) for early and delayed intubation.
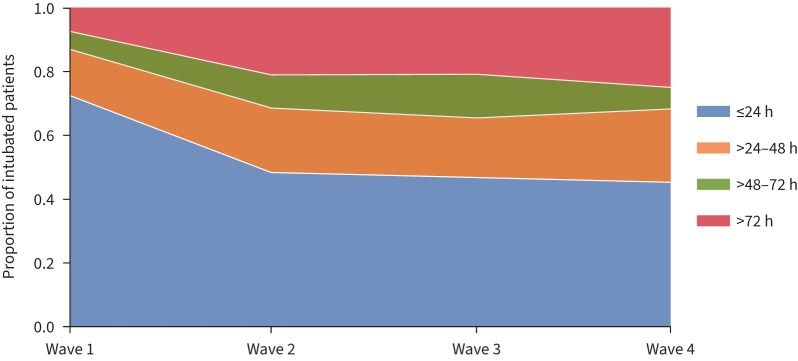
Results: Of the 2725 patients who received invasive mechanical ventilation, a total of 614 matched patients were included in the analysis (307 for each group). In the unmatched population, there were no differences in mortality between the early and delayed groups. After propensity score matching, patients with delayed intubation presented higher hospital mortality (27.3% versus 37.1%; p=0.01), ICU mortality (25.7% versus 36.1%; p=0.007) and 90-day mortality (30.9% versus 40.2%; p=0.02) compared with the early intubation group. Very similar findings were observed when we used a 48-h time-point for early or delayed intubation. The use of early intubation decreased after the first wave of the pandemic (72%, 49%, 46% and 45% in the first, second, third and fourth waves, respectively; first versus second, third and fourth waves p<0.001). In both the main and sensitivity analyses, hospital mortality was lower in patients receiving high-flow nasal cannula (HFNC) (n=294) who were intubated earlier. The subgroup of patients undergoing noninvasive ventilation (n=214) before intubation showed higher mortality when delayed intubation was set as that occurring after 48 h from ICU admission, but not when after 24 h.
Conclusions: In patients with COVID-19 requiring invasive mechanical ventilation, delayed intubation was associated with a higher risk of hospital mortality. The use of early intubation significantly decreased throughout the course of the pandemic. Benefits of such an approach occurred more notably in patients who had received HFNC.
Copyright ©The authors 2023.
Conflict of interest statement
Conflicts of interest: O. Roca discloses a research grant from Hamilton Medical AG; speaker fees from Hamilton Medical AG, Ambu, Fisher & Paykel Ltd and Aerogen Ltd; and nonfinancial research support from Timpel and Masimo. R. Mellado-Artigas reports speaker fees from Medtronic and Fisher & Paykel, all outside the submitted work. The remaining authors declare no conflicts of interest.
Figures