

Risk of atrial fibrillation and stroke among older men exposed to prolonged endurance sport practice: a 10-year follow-up. The Birkebeiner Ageing Study and the Tromsø Study
- PMID: 36396296
- PMCID: PMC9677011
- DOI: 10.1136/openhrt-2022-002154
Risk of atrial fibrillation and stroke among older men exposed to prolonged endurance sport practice: a 10-year follow-up. The Birkebeiner Ageing Study and the Tromsø Study
Abstract
Aims: Endurance sport practice is associated with a high prevalence of atrial fibrillation (AF), which increases the risk of stroke in the general population. However, stroke risk in endurance athletes with AF is sparsely investigated. Most studies have been limited by design and are largely restricted to younger and middle-aged populations. Thus, we aimed to investigate AF and stroke risk in older athletes exposed to prolonged endurance training.
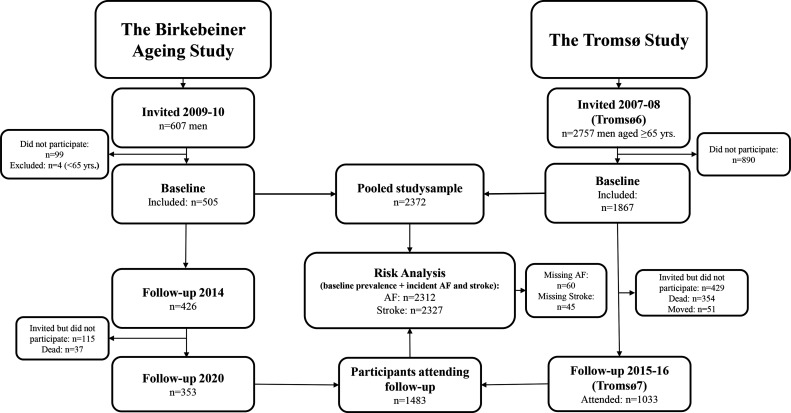
Method: During a 10-year period, 505 male athletes aged ≥65 years frequently participating in a long-distance ski race were compared with 1867 men of the same age from the general population. The main exposure was endurance sport practice with self-reported AF and stroke as outcomes. Stroke risk was further examined by joint modelling of AF and endurance practice. Statistical analysis was conducted with a modified Poisson model.
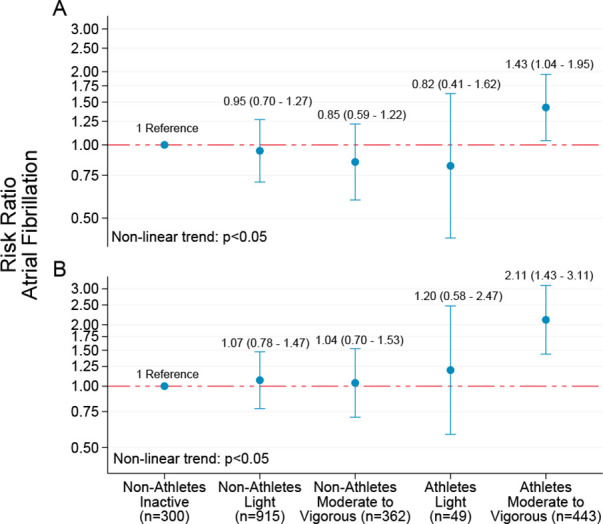
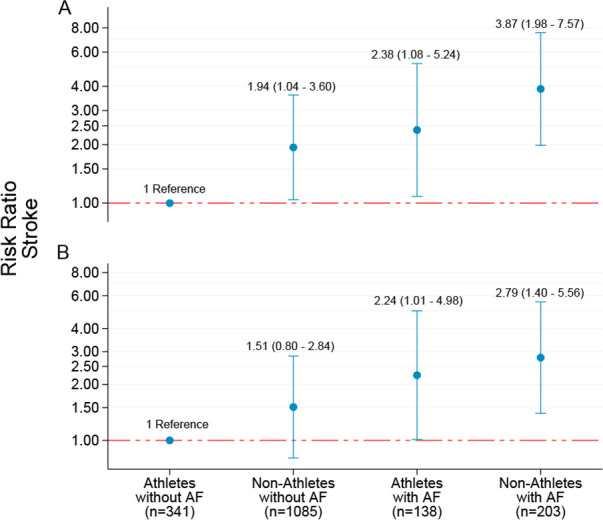
Results: Athletes (median age: 68, range: 65-90) participated in a long-distance ski race over a median of 14 years (range: 1-53). Prevalence (28.5% vs 17.8%) and adjusted risk of AF (risk ratio (RR): 1.88, 95% CI: 1.49 to 2.37) were higher in athletes compared with non-athletes, whereas the prevalence (5.4% vs 9.7%) and risk of stroke were lower (RR: 0.60, 95% CI: 0.37 to 0.95). Compared with athletes without AF, risk of stroke was twofold in athletes (RR: 2.38, 95% CI: 1.08 to 5.24) and nearly fourfold in non-athletes (RR: 3.87, 95% CI: 1.98 to 7.57) with AF.
Conclusion: Although older male endurance athletes experienced an increased risk of AF, the long-term risk of stroke was substantially reduced compared with non-athletes.
Keywords: atrial fibrillation; epidemiology; stroke.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: M-LL has received lecture fees from Bayer, Sanofi and BMS/Pfizer not related to this study. MM has received lecture fees from Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, mSD and Pfizer not related to this work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical