

Evidence, detailed characterization and clinical context of complement activation in acute multisystem inflammatory syndrome in children
- PMID: 36396679
- PMCID: PMC9670087
- DOI: 10.1038/s41598-022-23806-5
Evidence, detailed characterization and clinical context of complement activation in acute multisystem inflammatory syndrome in children
Abstract
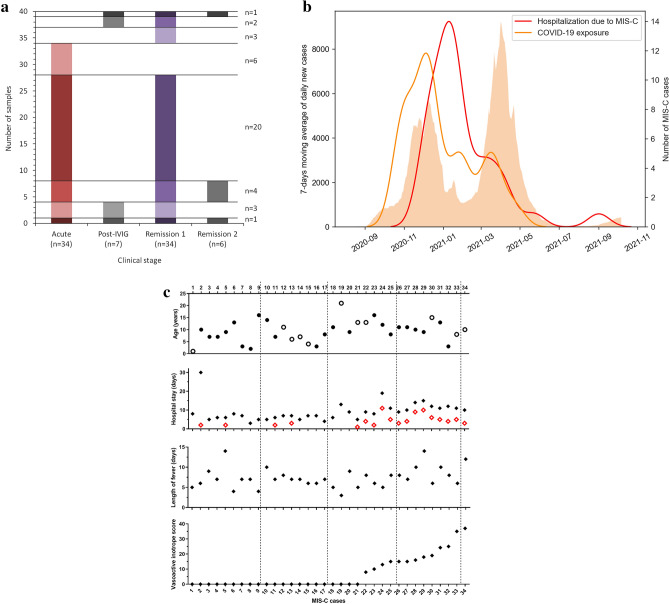
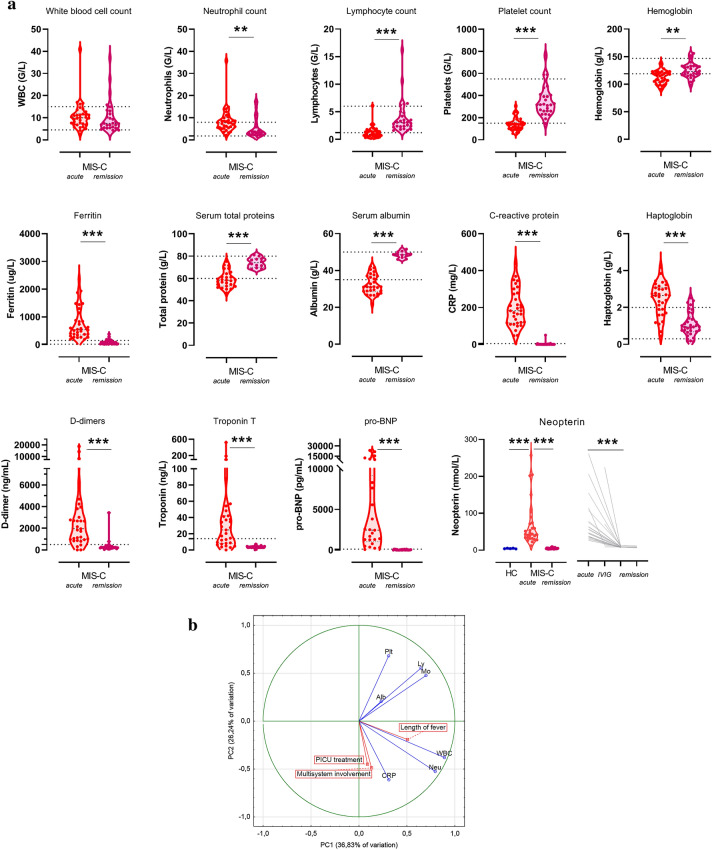
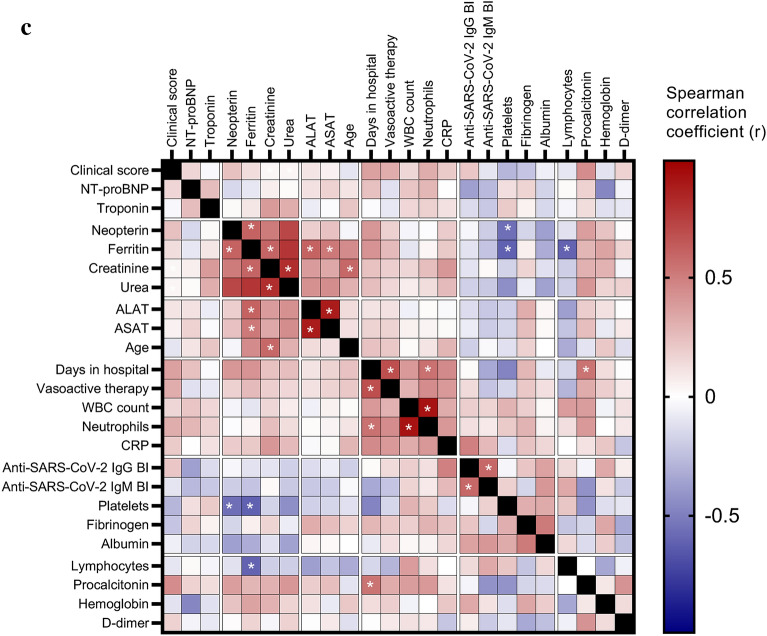
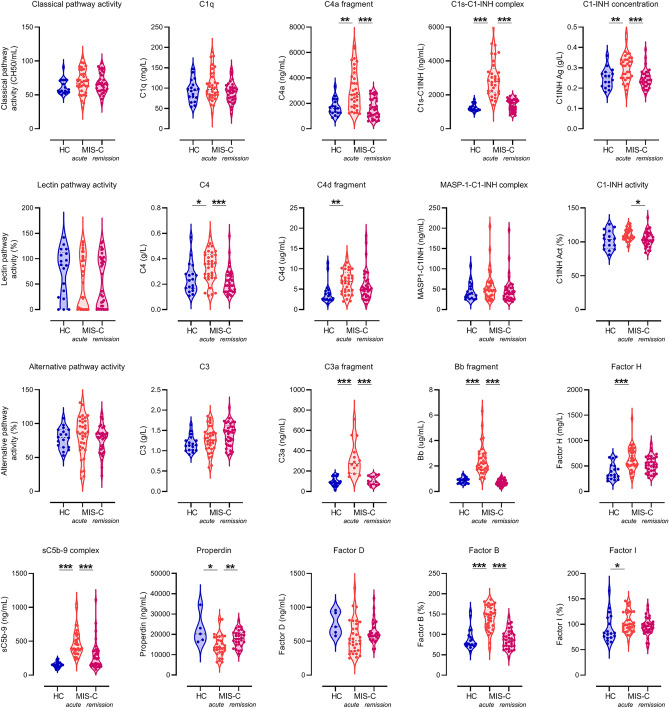
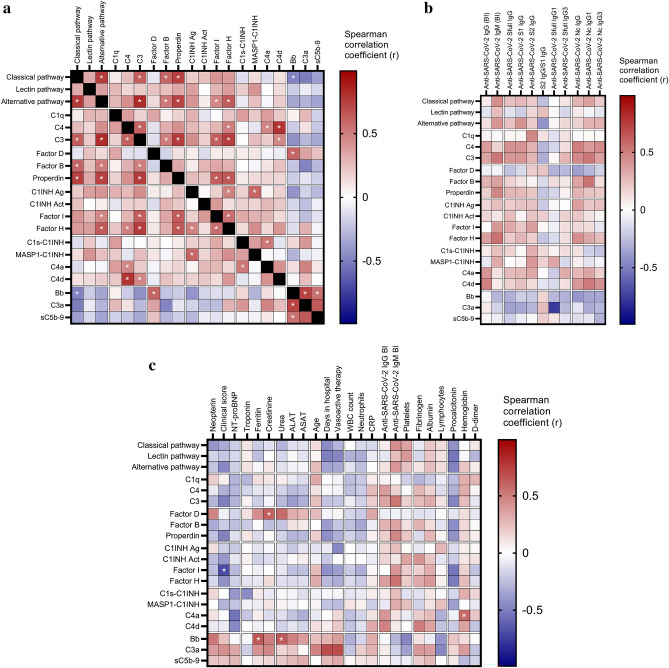
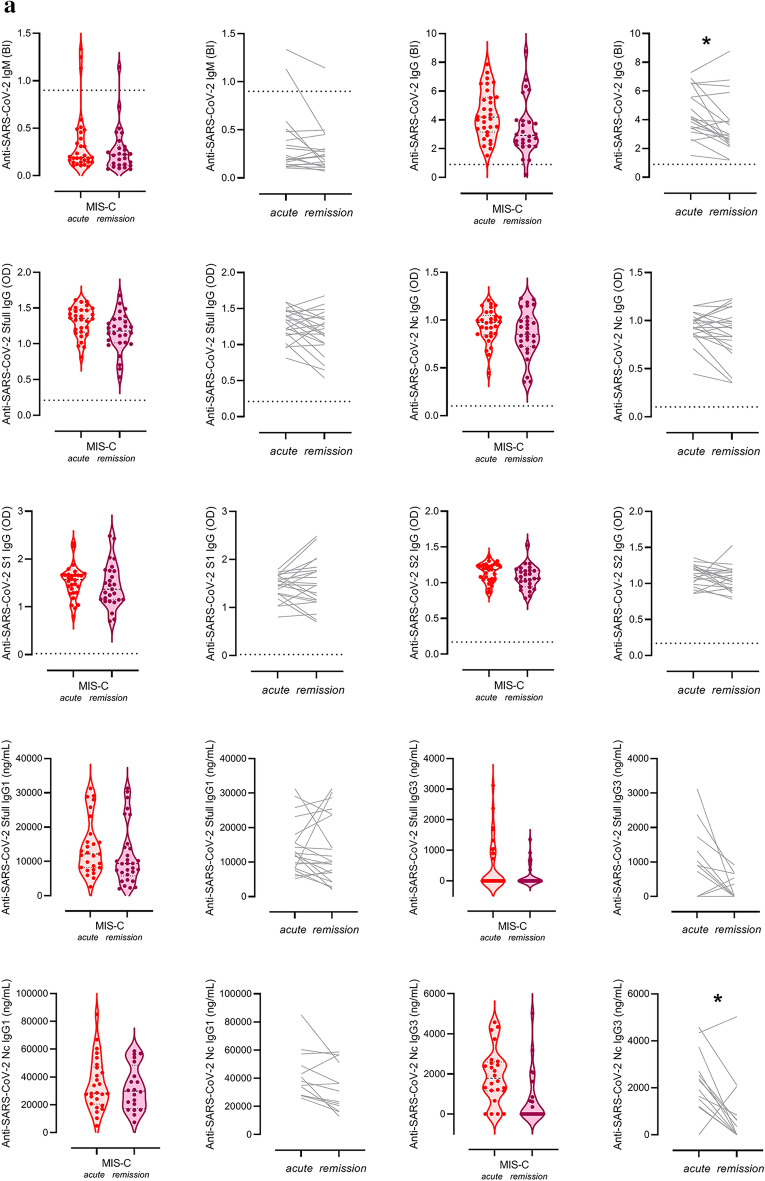
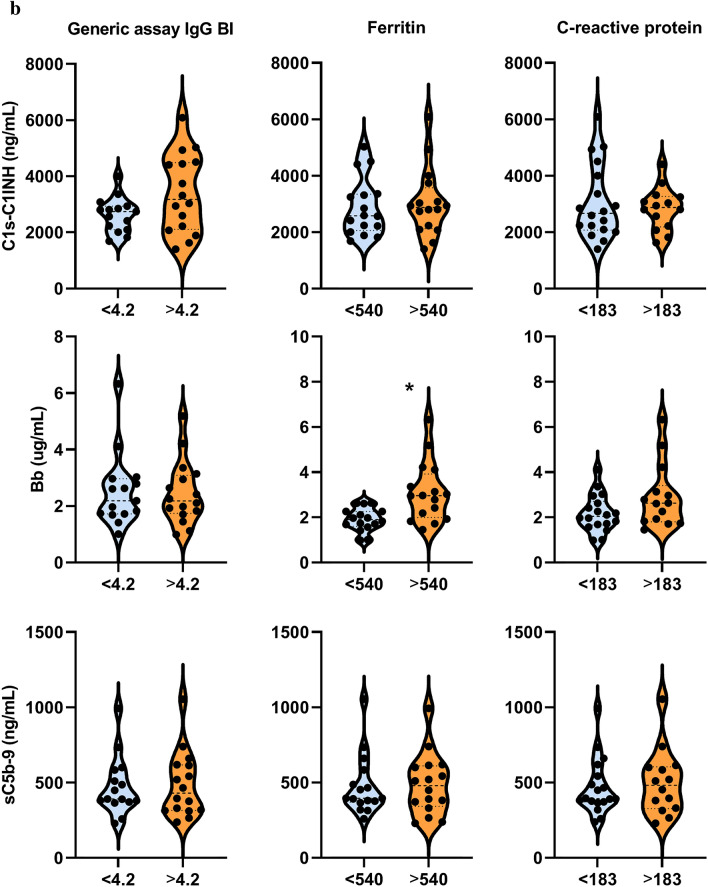
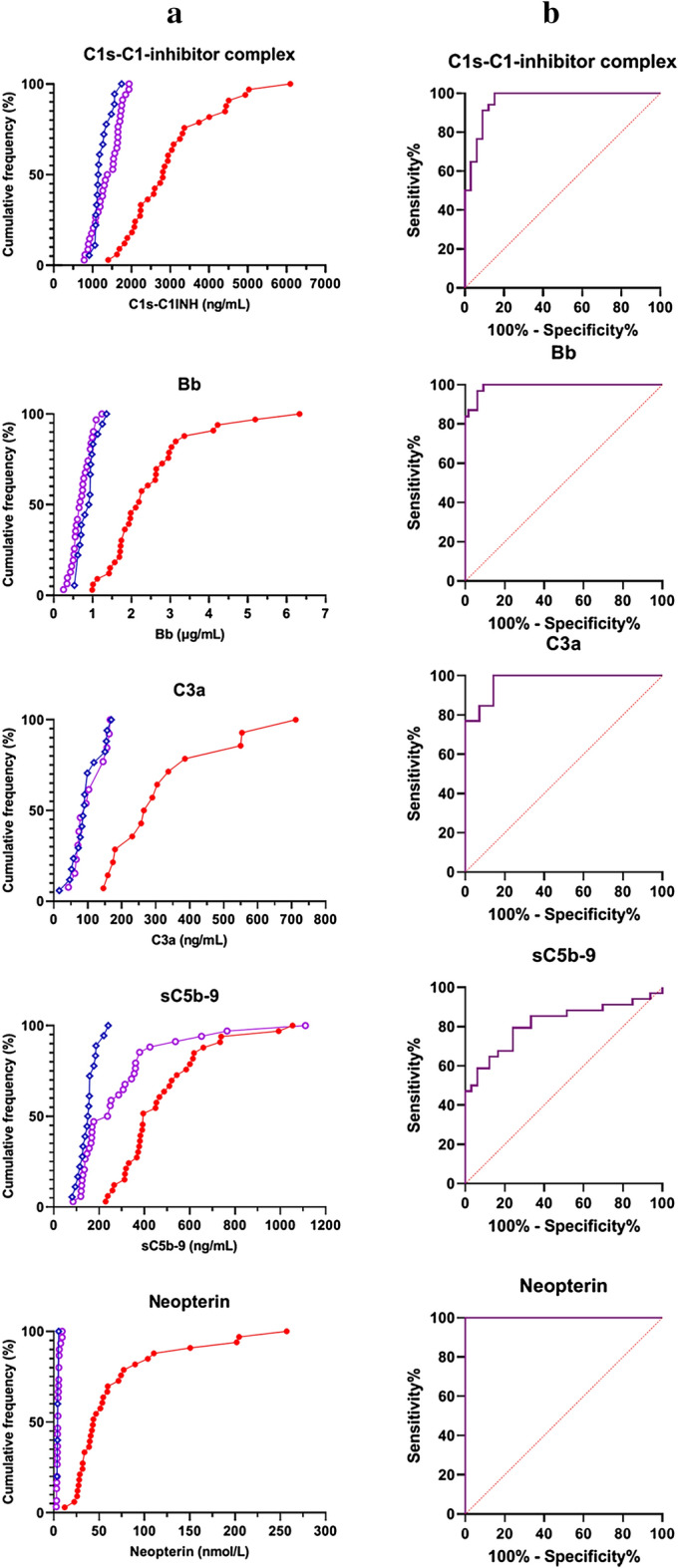
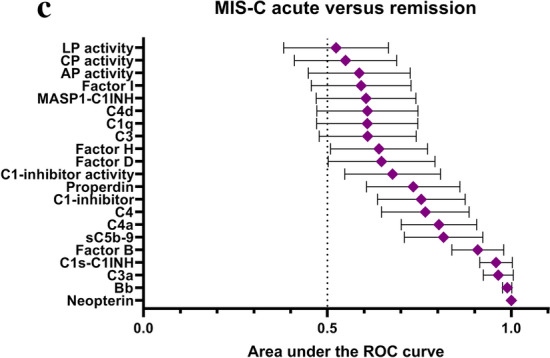
Multisystem inflammatory syndrome in children (MIS-C) is a rare, life-threatening complication of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. MIS-C develops with high fever, marked inflammation and shock-like picture several weeks after exposure to, or mild infection with SARS-CoV-2. Deep immune profiling identified activated macrophages, neutrophils, B-plasmablasts and CD8 + T cells as key determinants of pathogenesis together with multiple inflammatory markers. The disease rapidly responds to intravenous immunoglobulin (IVIG) treatment with clear changes of immune features. Here we present the results of a comprehensive analysis of the complement system in the context of MIS-C activity and describe characteristic changes during IVIG treatment. We show that activation markers of the classical, alternative and terminal pathways are highly elevated, that the activation is largely independent of anti-SARS-CoV-2 humoral immune response, but is strongly associated with markers of macrophage activation. Decrease of complement activation is closely associated with rapid improvement of MIS-C after IVIG treatment.
© 2022. The Author(s).
Conflict of interest statement
L. W. and E. T. are employees of Hycult Biotech. Other authors have no conflict of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
