

An interpretable RL framework for pre-deployment modeling in ICU hypotension management
- PMID: 36396808
- PMCID: PMC9671896
- DOI: 10.1038/s41746-022-00708-4
An interpretable RL framework for pre-deployment modeling in ICU hypotension management
Abstract
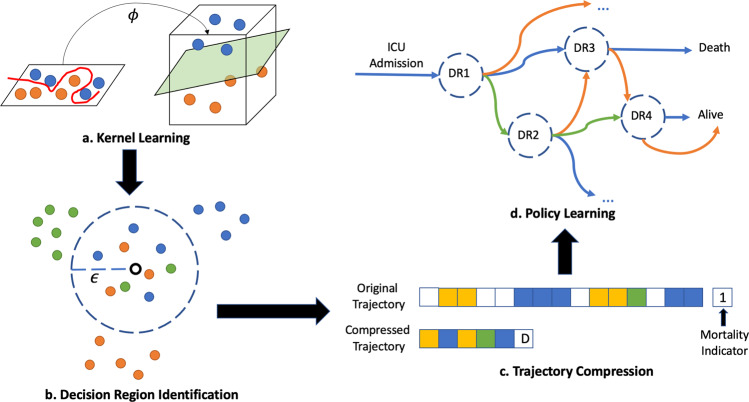
Computational methods from reinforcement learning have shown promise in inferring treatment strategies for hypotension management and other clinical decision-making challenges. Unfortunately, the resulting models are often difficult for clinicians to interpret, making clinical inspection and validation of these computationally derived strategies challenging in advance of deployment. In this work, we develop a general framework for identifying succinct sets of clinical contexts in which clinicians make very different treatment choices, tracing the effects of those choices, and inferring a set of recommendations for those specific contexts. By focusing on these few key decision points, our framework produces succinct, interpretable treatment strategies that can each be easily visualized and verified by clinical experts. This interrogation process allows clinicians to leverage the model's use of historical data in tandem with their own expertise to determine which recommendations are worth investigating further e.g. at the bedside. We demonstrate the value of this approach via application to hypotension management in the ICU, an area with critical implications for patient outcomes that lacks data-driven individualized treatment strategies; that said, our framework has broad implications on how to use computational methods to assist with decision-making challenges on a wide range of clinical domains.
© 2022. The Author(s).
Conflict of interest statement
The authors declare competing interests: F.D.V. consults for Davita Kidney Care. K.Z., H.W., J.D., B.C., L.A.C., and R.K. declare no competing interests.
Figures





References
-
- Yu, C., Liu, J., Nemati, S. & Yin, G. Reinforcement learning in healthcare: a survey. ACM Comput. Surv. 55, 5 (2021).
LinkOut - more resources
Full Text Sources
