

Cervical cancer heterogeneity: a constant battle against viruses and drugs
- PMID: 36397138
- PMCID: PMC9670454
- DOI: 10.1186/s40364-022-00428-7
Cervical cancer heterogeneity: a constant battle against viruses and drugs
Abstract
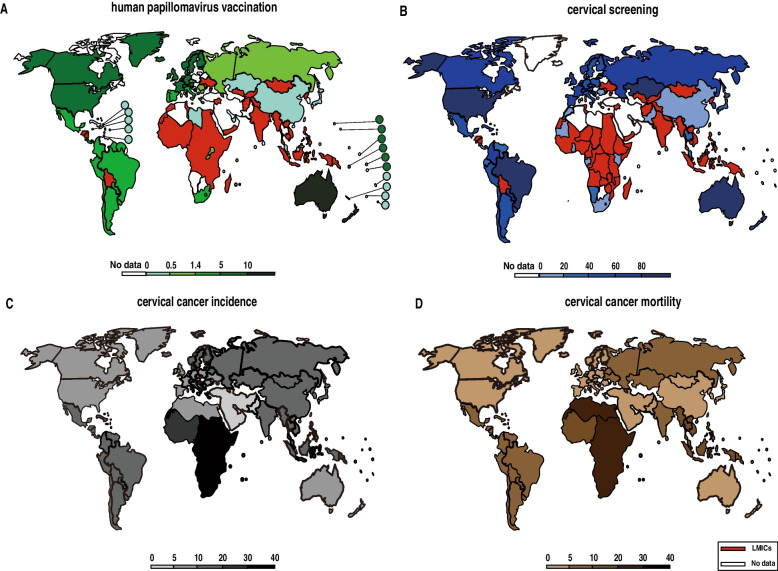
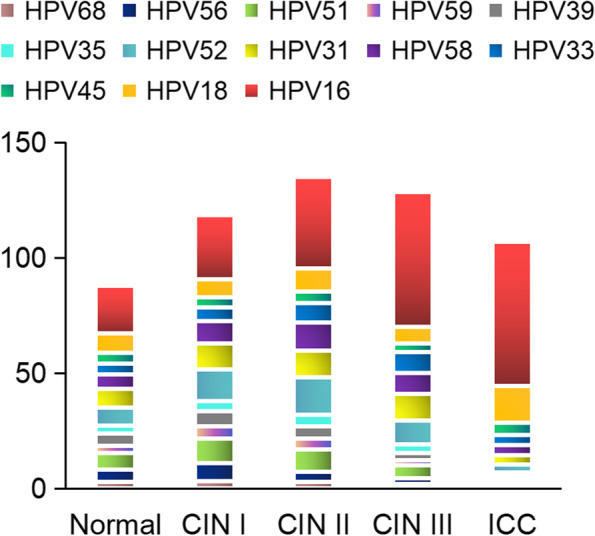
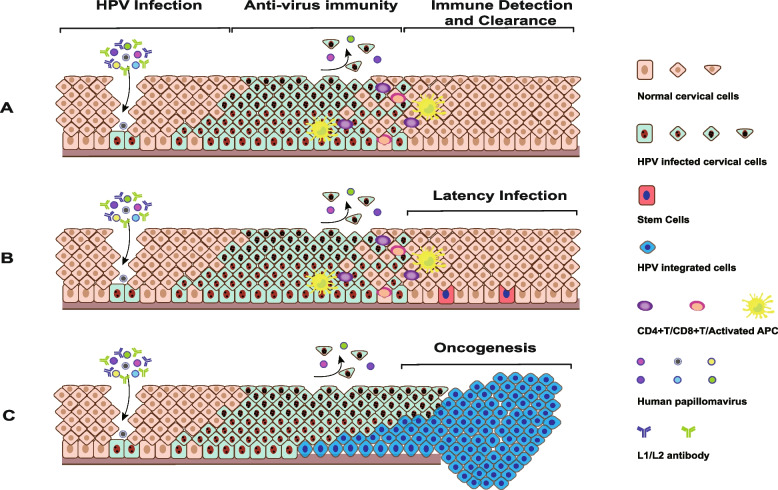
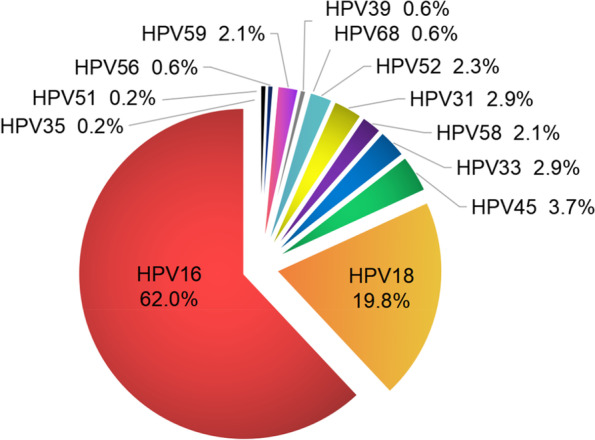
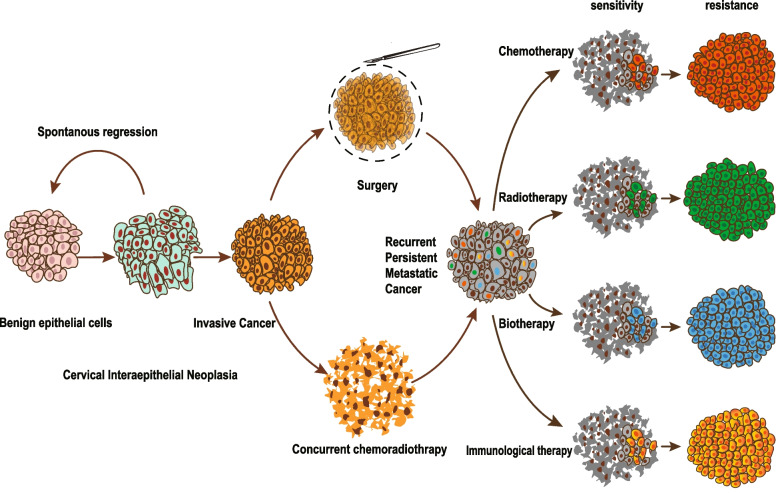
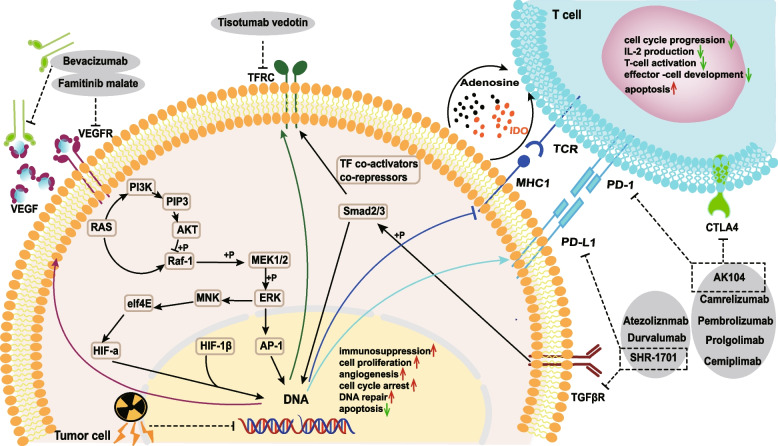
Cervical cancer is the first identified human papillomavirus (HPV) associated cancer and the most promising malignancy to be eliminated. However, the ever-changing virus subtypes and acquired multiple drug resistance continue to induce failure of tumor prevention and treatment. The exploration of cervical cancer heterogeneity is the crucial way to achieve effective prevention and precise treatment. Tumor heterogeneity exists in various aspects including the immune clearance of viruses, tumorigenesis, neoplasm recurrence, metastasis and drug resistance. Tumor development and drug resistance are often driven by potential gene amplification and deletion, not only somatic genomic alterations, but also copy number amplifications, histone modification and DNA methylation. Genomic rearrangements may occur by selection effects from chemotherapy or radiotherapy which exhibits genetic intra-tumor heterogeneity in advanced cervical cancers. The combined application of cervical cancer therapeutic vaccine and immune checkpoint inhibitors has become an effective strategy to address the heterogeneity of treatment. In this review, we will integrate classic and recently updated epidemiological data on vaccination rates, screening rates, incidence and mortality of cervical cancer patients worldwide aiming to understand the current situation of disease prevention and control and identify the direction of urgent efforts. Additionally, we will focus on the tumor environment to summarize the conditions of immune clearance and gene integration after different HPV infections and to explore the genomic factors of tumor heterogeneity. Finally, we will make a thorough inquiry into completed and ongoing phase III clinical trials in cervical cancer and summarize molecular mechanisms of drug resistance among chemotherapy, radiotherapy, biotherapy, and immunotherapy.
Keywords: Drug resistance; Human papillomavirus; Immunotherapy; Tumor heterogeneity; Tumor microenvironment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Pett M, Coleman N. Integration of high-risk human papillomavirus: a key event in cervical carcinogenesis? J Pathol. 2007;212(4):356–367. - PubMed
-
- Castellsague X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol Oncol. 2008;110(3 Suppl 2):S4–7. - PubMed
-
- Cook OF. The Mendelian Inheritance of Mutations. Science. 1908;28(707):86–88. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
