

The value of the sacroiliac joint area as a new morphological parameter of ankylosing spondylitis
- PMID: 36397357
- PMCID: PMC9666185
- DOI: 10.1097/MD.0000000000031723
The value of the sacroiliac joint area as a new morphological parameter of ankylosing spondylitis
Abstract
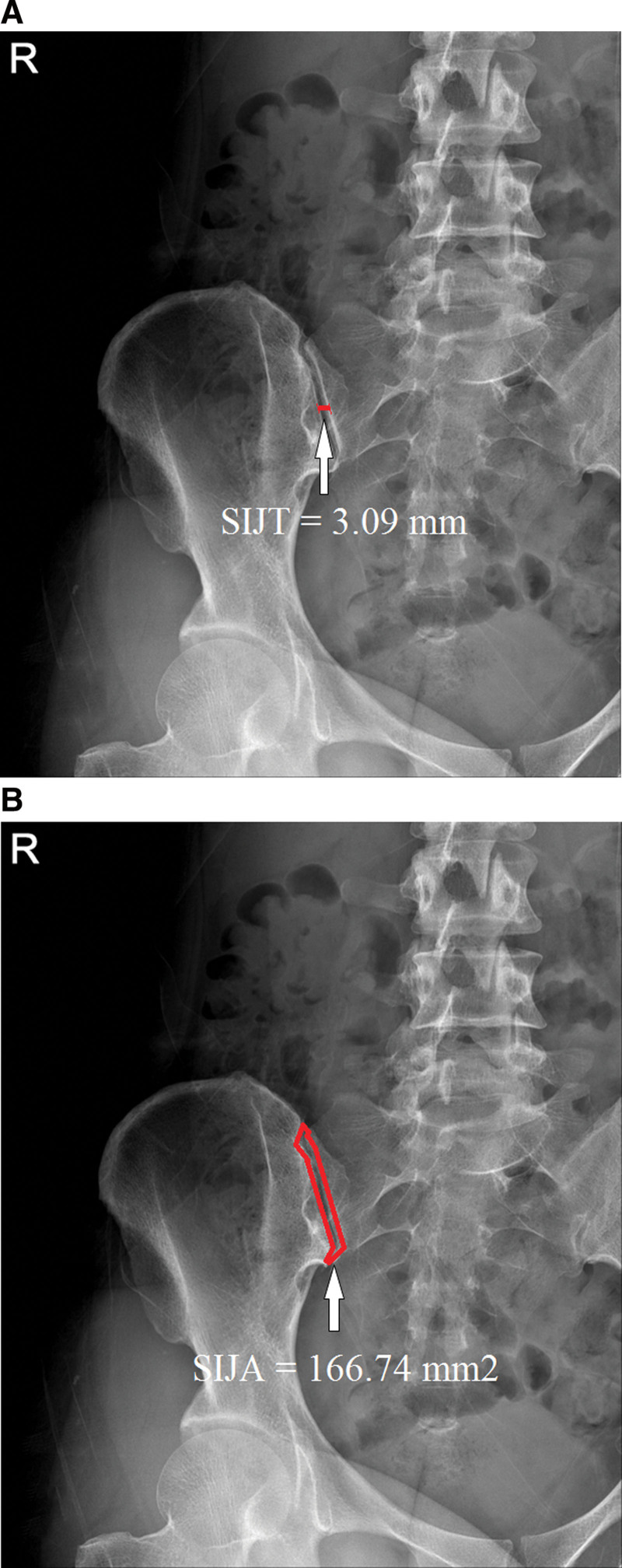
A narrowed sacroiliac joint (SIJ) space has been considered to be a major morphologic parameter of ankylosing spondylitis (AS). Previous studies revealed that the sacroiliac joint thickness (SIJT) correlated with AS in patients. However, irregular narrowing is different from thickness. Thus, we devised a method using the sacroiliac joint cross-sectional area (SIJA) as a new morphological parameter for use in evaluating AS. We hypothesized that the SIJA is a key morphologic parameter in diagnosing AS. SIJ samples were collected from 107 patients with AS, and from 85 control subjects who underwent SIJ-view X-rays that revealed no evidence of AS. We measured the SIJT and SIJA at the SIJ margin on X-rays using our picture archiving and communications system. The SIJT was measured at the narrowest point between the sacrum and the ilium. The SIJA was measured as the entire cross-sectional joint space area of the SIJ in the X-ray images. The average SIJT was 3.09 ± 0.61 mm in the control group, and 1.59 ± 0.52 mm in the AS group. The average SIJA was 166.74 ± 39.98 mm2 in the control group, and 68.65 ± 24.11 mm2 in the AS group. AS patients had significantly lower SIJT (P < .001) and SIJA (P < .001) than the control subjects. Receiver operating characteristics curve analysis showed that the best cutoff point for the SIJT was 2.33 mm, with 92.5% sensitivity, 94.1% specificity, and an area under the curve of 0.97 (95% confidence interval: 0.95-0.99). The optimal cutoff point for the SIJA was 106.19 mm2, with 93.5% sensitivity, 95.3% specificity, and an area under the curve of 0.98 (95% confidence interval: 0.97-1.00). Although the SIJT and SIJA were both significantly associated with AS, the SIJA parameter was a more sensitive measurement. We concluded that the SIJA is an easy-to-use, fast, cheap, and useful new morphological parameter for predicting AS.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Sharan D, Rajkumar JS. Physiotherapy for ankylosing spondylitis: systematic review and a proposed rehabilitation protocol. Curr Rheumatol Rev. 2017;13:121–5. - PubMed
