

Which is the best way for patients with ureteral obstruction? Percutaneous nephrostomy versus double J stenting
- PMID: 36397363
- PMCID: PMC9666138
- DOI: 10.1097/MD.0000000000031194
Which is the best way for patients with ureteral obstruction? Percutaneous nephrostomy versus double J stenting
Abstract
Background: Percutaneous nephrostomy (PCN) and Double J stenting (DJS) are the 2 main treatment options of ureteral obstruction. We evaluate which of these 2 methods is superior concerning the course of procedure, postoperative complication and quality of life.
Methods: A detailed review of electronic databases including PubMed, Embase, Cochrane Library, China Biology Medicine disc, China National Knowledge Infrastructure up to February 21st, 2021 was searched. Continuous data were evaluated using mean difference (MD) with 95% confidence interval (CI), while nominal data were analyzed by risk ratio (RR) with 95% CI. Meanwhile, we performed the subgroup analysis based on study design, disease type, sample size, sepsis, DJ diameter, nephrostomy diameter, anesthesia type and guidance under X-ray or ultrasound.
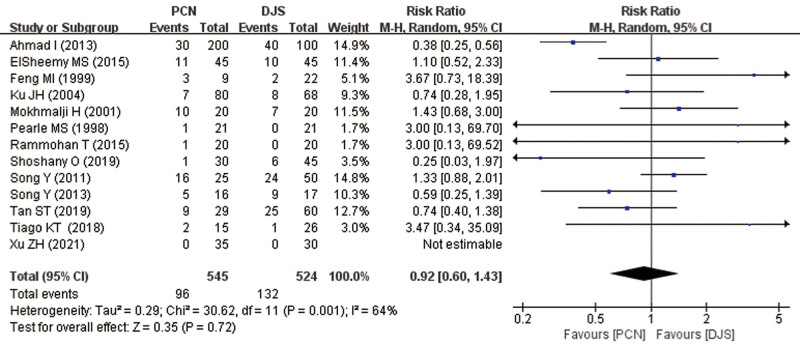
Results: There were 18 previous studies included in current study. As a result, we found that there were significant differences in fluoroscopy time (MD = 0.31; 95% CI, 0.14-0.48, P < .001) and hospital stay (MD = 1.23; 95% CI, 0.60-1.85, P < .001). However, no statistic difference was detected in operative time (MD = 5.40; 95% CI, -1.78 to 12.58, P = .140) between the paired groups. Although DJS showed a higher rate of postoperative complications (25.19% vs 17.61%), there was no significant difference in the incidence of complications following DJS and PCN (RR = 0.92; 95% CI, 0.60-1.43; P = .720). Based on the EuroQol analysis, the 2 main treatment options had different impacts on quality of life. The pooled results showed that PCN patients reported more difficulties in self-care compared to DJS patients (RR = 3.07; 95% CI, 1.32-7.14; P = .009).
Conclusions: DJS is a safe and better method of temporary urinary diversion than PCN for management of ureteral obstruction with shorter fluoroscopy time and hospital stay. As for quality of life, patients receiving PCN had a distinct difficulty in self-care compared to those receiving DJS. However, these 2 treatment options often depends on the individual situation.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures





References
-
- Tabib C, Nethala D, Kozel Z, et al. . Management and treatment options when facing malignant ureteral obstruction. Int J Urol. 2020;27:591–8. - PubMed
-
- Netsch C, Becker B, Gross AJ. Therapie der Harnleiterobstruktion: Stellenwert von perkutaner Nephrostomie und von Harnleiterschienen [Management of ureteral obstruction: value of percutaneous nephrostomy and ureteral stents]. Urologe A. 2016;55:1497–510. - PubMed
-
- Hardie EM, Kyles AE. Management of ureteral obstruction. Vet Clin North Am Small Anim Pract. 2004;34:989–1010. - PubMed
-
- Munafo MR, Flint J. Meta-analysis of genetic association studies. Trends Genet. 2004;20:439–44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
