

Analysis of the status quo of pelvic floor muscle and the effect of pelvic floor muscle training in second pregnant women
- PMID: 36397372
- PMCID: PMC9666209
- DOI: 10.1097/MD.0000000000031370
Analysis of the status quo of pelvic floor muscle and the effect of pelvic floor muscle training in second pregnant women
Abstract
Objective: This study aims to investigate the current situation of pelvic floor muscle (PFM) in the second trimester postpartum 42 days by detecting the electrophysiological indexes of PFM on pelvic floor rehabilitation after 2 months.
Methods: In total, 198 cases of second child puerpera were selected, who were delivered in our hospital between June 1, 2020, and December 10, 2020, and underwent outpatient reexamination 42 days after delivery.
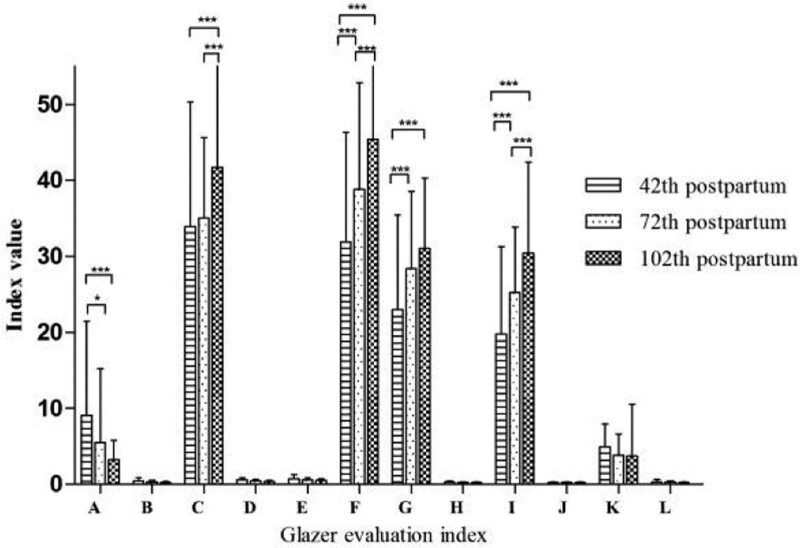
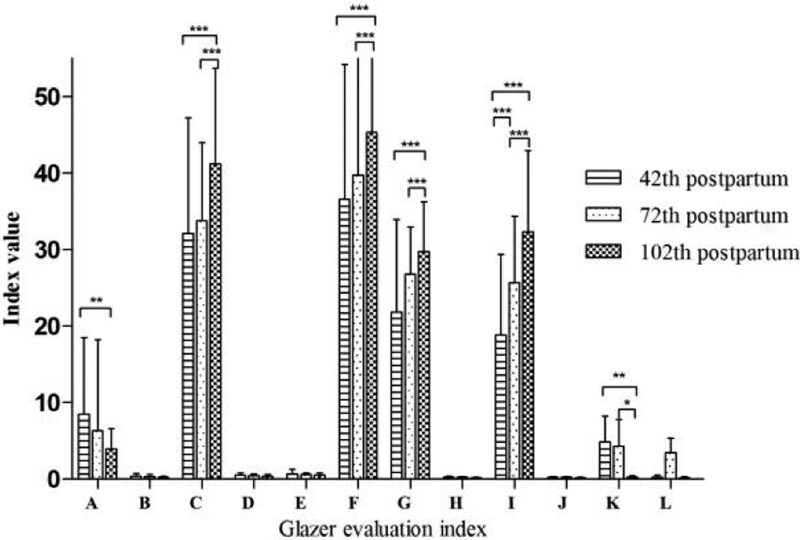
Results: Except for the rest post-baseline stage values, the pelvic floor surface electromyography evaluation values significantly differed from each other at the considered time points in group A, P < .05; on day 72 in group B, no obvious improvement in the evaluation values was observed as than those on day 42 (P > .05) except for the endurance contractions stage values. However, on day 102, all values were markedly different at each considered time point (P < .05). On day 102 postpartum, the evaluation values of group A in the rest pre-baseline stage, the time before and after peak of phasic (flick) contractions stage, and the endurance contractions stage were significantly improved to those in group B with all P < .05. On day 42 after parturition, each index of the tonic contractions stage was higher after spontaneous labor than that after cesarean; the differences were all significant, P < .05, but on day 102 postpartum, all of the values exhibited no difference between the 2 modes. In only the phasic (flick) contractions stage at 42th, were the values of younger mothers obviously higher, P = .025; the other stage values for different ages of women during different time periods were not statistically significant, P > .05.
Conclusions: In the short term, the effect of biofeedback plus electrical stimulation on the PFM function in second pregnant women was better than that of the Kegel exercise, but with time, there was no significant difference between the 2 training methods on the recovery of the PFM.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Effect of different delivery modes on the short-term strength of the pelvic floor muscle in Chinese primipara.BMC Pregnancy Childbirth. 2018 Jul 3;18(1):275. doi: 10.1186/s12884-018-1918-7. BMC Pregnancy Childbirth. 2018. PMID: 29970030 Free PMC article.
-
The effect of water immersion delivery on the strength of pelvic floor muscle and pelvic floor disorders during postpartum period: An experimental study.Medicine (Baltimore). 2017 Oct;96(41):e8124. doi: 10.1097/MD.0000000000008124. Medicine (Baltimore). 2017. PMID: 29019880 Free PMC article.
-
Effect of health education combined with biofeedback electrical stimulation on early pelvic floor function and psychology: A retrospective study.Medicine (Baltimore). 2024 Aug 23;103(34):e39321. doi: 10.1097/MD.0000000000039321. Medicine (Baltimore). 2024. PMID: 39183430 Free PMC article.
-
[Postpartum pelvic floor rehabilitation on prevention of female pelvic floor dysfunction: a multicenter prospective randomized controlled study].Zhonghua Fu Chan Ke Za Zhi. 2015 Jun;50(6):420-7. Zhonghua Fu Chan Ke Za Zhi. 2015. PMID: 26311549 Clinical Trial. Chinese.
-
Improving the Technique of Pelvic Floor Muscle Contraction in Active Nulliparous Women Attending a Structured High-Low Impact Aerobics Program-A Randomized Control Trial.Int J Environ Res Public Health. 2022 May 12;19(10):5911. doi: 10.3390/ijerph19105911. Int J Environ Res Public Health. 2022. PMID: 35627446 Free PMC article. Clinical Trial.
Cited by
-
Effects of Kegel exercise combined with rational emotive behavior therapy on pelvic floor muscle function and sexual life quality in patients with total hysterectomy: A retrospective study.Medicine (Baltimore). 2023 Dec 29;102(52):e36222. doi: 10.1097/MD.0000000000036222. Medicine (Baltimore). 2023. PMID: 38206697 Free PMC article.
References
-
- Zhu L, Lang JH. Female pelvisology. Beijing: People’s Medical Publishing House. 2008: 22– 33.
-
- Lawson S, Sacks A. Pelvic floor physical therapy and women’s health promotion. J Midwifery Womens Health. 2018;63:410417. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
